With Need Rising, Medicaid Is at Risk for Cuts
With millions of Americans newly unemployed or facing sharp income losses, the need for Medicaid coverage is growing. While comprehensive data are not yet available, preliminary data for a subset of states show enrollment is rising, Georgetown Center for Children and Families analysis finds.[1] Among 22 states with June data, enrollment is up 6.6 percent since February. Among non-elderly adults enrolled through the Affordable Care Act’s (ACA) Medicaid expansion, a group particularly likely to need Medicaid due to the recession, enrollment is up almost 10 percent since February in 15 states with available data. If unemployment remains above 10 percent through the end of this year, as the Congressional Budget Office (CBO) projects, non-elderly Medicaid enrollment will likely rise by 9 to 16 percent compared to pre-crisis levels, or by 5 to 8 million people, Urban Institute projections indicate. State Medicaid programs are also taking steps — and incurring costs — to respond to COVID-19.
"The growing need for Medicaid coincides with a major state budget crisis."The growing need for Medicaid coincides with a major state budget crisis. States budget shortfalls are projected to total $555 billion through state fiscal year 2022, largely because revenues have fallen precipitously and will not recover until the virus is under control and economic activity rebounds. Federal policymakers acted quickly in March to provide additional Medicaid funding and institute protections that keep states from cutting eligibility or taking away coverage from current enrollees. Even so, a number of states have made or are considering Medicaid cuts, including reductions in provider payments, reversals of planned and needed coverage improvements, and furloughs and hiring freezes impacting eligibility workers. States are also cutting behavioral health programs, and, even in the midst of a pandemic, are cutting their public health budgets.
With the state budget crisis intensifying and states beginning to exhaust their options to defer budget cuts, they will likely make deeper and more widespread cuts to Medicaid and other health programs unless federal policymakers provide additional funds and maintain strong protections for Medicaid enrollees.
Need for Medicaid Coverage Increasing
Medicaid enrollment rises in recessions, as people who lose their jobs or lose income become eligible and need coverage. Drawing on experience from past recessions, Urban Institute researchers project that, with unemployment at 15 percent, non-elderly Medicaid enrollment would ultimately rise by 16 to 29 percent, or 8 to 14 million people. With unemployment at 10 percent, the increase would be about 9 to 16 percent, or 5 to 8 million people. CBO projects that unemployment will peak at 14 percent in the third quarter of this year and remain above 10 percent through the end of 2020.[2]
Medicaid enrollment increases typically lag behind increases in people receiving unemployment insurance (UI) or SNAP (food stamp) benefits, because people losing jobs or income often focus on their most urgent needs (like food and rent) first, and because people do not always lose job-based coverage immediately upon losing a job.[3] For example, while Medicaid enrollment rose by over 20 percent in the two years after the December 2007 start of the Great Recession, only a small fraction of that growth materialized after one year, compared to a much larger share of total growth in UI and SNAP enrollment.[4] During the current crisis, Medicaid enrollment may lag even further, because COVID-19 has led people to defer non-urgent medical visits, which are often an impetus to enroll in coverage, especially since providers can help people apply.
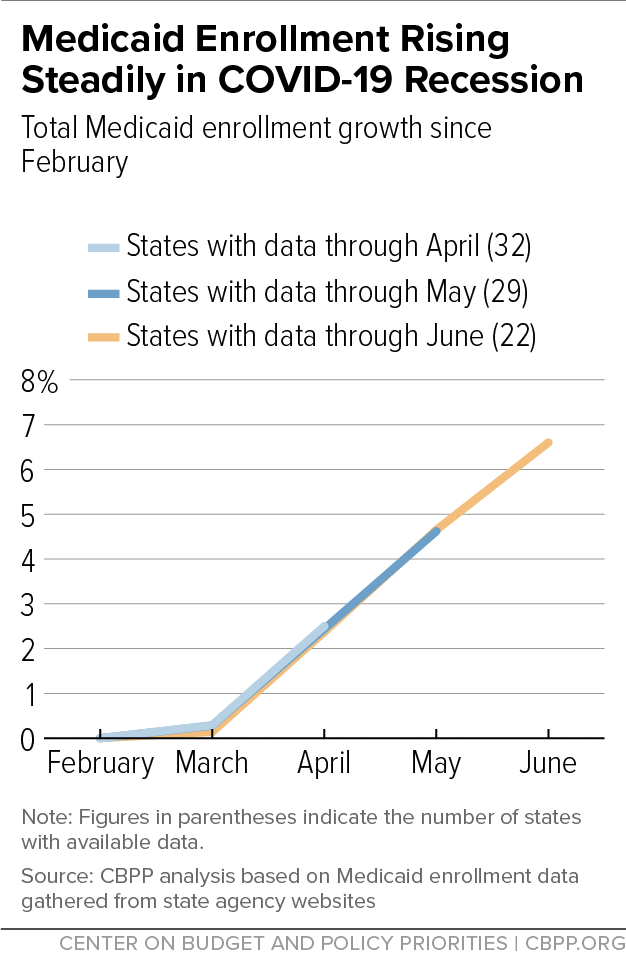
Nonetheless, enrollment is rising, data from a subset of states show.[5] The data are preliminary and may differ from figures that the Centers for Medicare & Medicaid Services (CMS) will release in the coming months; in some cases, they also cover only a subset of enrollees (such as those enrolled through managed care plans). Still, the available data show clearly that the recession is driving enrollment growth, and growth has accelerated since the first months of the downturn.[6] (See Figure 1. The appendix provides data for individual states and explains the limitations of that data.)
Before the pandemic and recession, Medicaid enrollment was flat or falling nationally and in most states.[7] In recent months:
- Across 32 states that report enrollment for all or most enrollees through April, enrollment rose by 2.5 percent between February and April.
- Across 29 states that report enrollment data for all or most enrollees through May, enrollment rose by 2.4 percent through April and 4.6 percent through May.
- Across 22 states that report enrollment data for all or most enrollees through June, enrollment rose by 2.4 percent through April, 4.7 percent through May, and 6.6 percent through June. In these states alone, accounting for roughly two-fifths of total pre-crisis Medicaid enrollment, enrollment has risen by 2.0 million people.

These data include groups for whom enrollment is generally not as responsive to economic conditions, such as elderly people and people with disabilities who are enrolled in both Medicare and Medicaid. Enrollment increases among adults covered through the ACA’s Medicaid expansion have been much larger, with Medicaid serving as a safety net as millions of adults have lost jobs or income. Among the 15 states for which we have data through June, for example, expansion enrollment had risen by 3.3 percent through April, 6.5 percent through May, and 9.8 percent through June.[8] (See Figure 2.) Among 18 states for which we have data through May, enrollment rose 7.1 percent between February and May.
Many state Medicaid programs are also implementing new policies in response to the pandemic, such as policies to maintain access to physical and behavioral health care while people are social distancing and policies to support health providers who have experienced large revenue declines as people defer non-emergency care. Some of these policies are increasing state costs, on top of the cost increases associated with growing enrollment.[9]
State Budget Crisis Puts Coverage and Access to Care at Risk
The growing need for Medicaid coincides with an unprecedented state budget crisis. States are facing estimated cumulative budget shortfalls of $555 billion from state fiscal years 2020 to 2022.[10] Without adequate federal aid and continued federal protections for beneficiaries, many states will likely enact Medicaid and other health care cuts that would jeopardize coverage and access to care in the midst of a public health crisis.
In March, federal policymakers took an important first step to address states’ fiscal challenges by enacting a 6.2 percentage-point increase in the federal medical assistance percentage, or FMAP — the share of Medicaid costs that the federal government pays in each state — as part of the Families First Coronavirus Response Act (Families First). The FMAP increase will remain in effect through the end of the official public health emergency and will provide about $40 billion in additional federal funding for each year that it remains in place.[11]
While the FMAP increase is small compared to total estimated state budget shortfalls, it has given states crucial immediate relief. States have used the increase to help close 2020 and 2021 budget shortfalls while avoiding or limiting Medicaid and other cuts. In Arizona, California, Georgia, Louisiana, Nevada, and Utah, state policymakers specifically noted in recent budget documents that the enhanced FMAP either helped preserve and protect their Medicaid programs or freed up state funds to avoid other cuts.[12]
Also important, Families First conditioned a state’s receipt of its additional federal funding on maintenance of effort (MOE) requirements, which have helped protect coverage by prohibiting states from cutting Medicaid eligibility, creating new barriers to coverage, or ending coverage for current beneficiaries while receiving the additional federal funds.
Medicaid Cuts Show Additional Federal Assistance Is Needed
Even so, a number of states have cut Medicaid or cancelled or delayed planned improvements, or are considering doing so. For example:
- California: The state reversed its plans to extend Medicaid coverage to seniors who would otherwise be eligible except for their immigration status, and it also delayed planned delivery system reforms and improvements in care coordination.[13] The state also enacted broad cuts to Medicaid provider rates that will take effect next year depending on state budget conditions, and Governor Gavin Newsom cautioned that without additional federal funding, the state will have to cut reimbursement rates to providers and optional Medicaid services.[14]
- Colorado: Colorado adopted a 1.0 percent cut in payments to Medicaid community providers, such as physicians and outpatient clinics, and cut payments to children’s and teaching hospitals. It also cut dental benefits, increased copayments, and delayed planned customer service improvements.[15]
- Florida: Governor Ron DeSantis vetoed increases in Medicaid payment rates for certain providers of services to people with disabilities that the legislature passed in March.[16]
- Nevada: Nevada adopted a 6 percent across-the-board cut in payment rates for hospitals, physicians, behavioral health providers, and long-term support services providers such as nursing homes.[17]
- Utah: Utah reversed plans to improve coverage by providing 12-month continuous eligibility for Medicaid to children up to age 6. It also cut outpatient hospital payment rates, payment rates for Medicaid Accountable Care Organizations, and Medicaid fee-for-service rates for some behavioral health services.[18]
- Tennessee: Tennessee reversed plans to seek a federal waiver to provide Medicaid coverage for a full year after a woman gives birth (instead of 60 days). It also reversed plans to extend dental coverage for pregnant and postpartum women, and to expand access to services for people with intellectual and developmental disabilities.[19]
- Washington: The state health agency is exploring cuts to Medicaid services such as adult dental coverage and school-based services and eliminating Medicaid coverage for certain immigrants.[20]
This list of cuts does not include furloughs or hiring freezes for state workers, which may include workers who process Medicaid eligibility. Nevada’s enacted budget requires most state employees to take 48 hours of unpaid furlough leave between January and July of 2021.[21] California,[22] New Jersey,[23] and Washington[24] are also planning to furlough some state workers, and states including Maryland,[25] New Mexico,[26] Ohio,[27] Tennessee,[28] and Virginia[29] have imposed broad hiring freezes. Especially with Medicaid application volumes rising due to the recession, furloughing or freezing hiring for eligibility workers could create application backlogs that delay coverage and access to care.
The cuts that states are already making underscore the need for additional federal funds for state Medicaid programs and for continuing the strong beneficiary protections of Families First. Although a good first step, the Families First FMAP increase is much smaller than the FMAP increases that policymakers enacted during the Great Recession, even though unemployment is currently, and is projected to remain, higher, and other federal aid for states that policymakers have enacted to date totals a small fraction of projected state shortfalls.[30] During past economic downturns and state budget crises, many states eliminated or cut benefits and provider payments. As Figure 3 shows, during the early 2000s, many states also cut eligibility or made it harder for eligible people to get and stay covered; during the Great Recession and its aftermath, federal MOE protections largely prohibited these cuts.
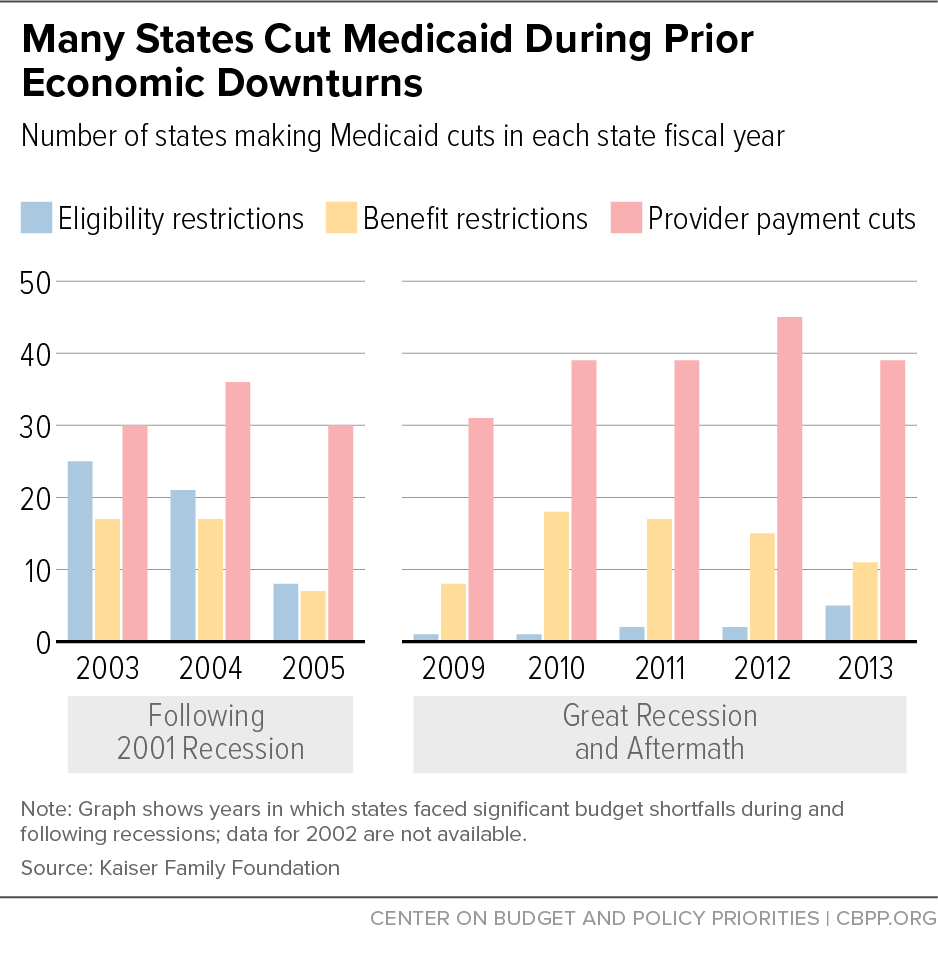
If policymakers do not provide additional federal aid, or weaken or eliminate MOE protections, states will likely make similar cuts going forward.[31] Such cuts would have especially devastating impacts during a recession that coincides with a public health crisis, and at a time when many health providers that serve Medicaid enrollees are already losing significant revenue because of a sharp drop in patient visits due to the pandemic.
States Also Cutting Non-Medicaid Health Programs
States are also cutting their non-Medicaid health programs. During the Great Recession, state-funded behavioral health programs were often targeted for cuts, with roughly 3 in 4 states cutting mental health budgets in each of 2009, 2010, and 2011.[32] The same seems to be occurring already in this recession, even as overdose deaths surge and many health experts have raised concerns about the impact of the pandemic and measures to control it on mental health.[33] For example:
- Colorado: Colorado cut funding for behavioral health programs, including a program designed to keep people with mental illness out of the hospital, a program providing mental health services for youth and adults in the correctional system, substance use treatment in county jails, and addiction treatment programs for underserved communities.[34]
- Florida: Governor Ron DeSantis vetoed funding that the state legislature provided for programs and services related to behavioral health, including opioid and other substance use treatment services, crisis intervention services, and services for people experiencing homelessness.[35]
- Georgia: The state cut spending for child, adolescent, and adult mental health services, including prevention programs, employment services, and housing vouchers for people with mental illness. It also cut substance use disorder services and services for adults with developmental disabilities.[36]
- Utah: The state cut funding for mental health and opioid use disorder services.[37]
- Washington: The state health agency is exploring cuts to substance use disorder services and other behavioral health programs.[38]
States have also cut their public health budgets and staffing, despite the public health crisis, with a Kaiser Health News analysis finding that at least 14 states have cut, or are seriously considering cutting, their public health budgets or staffing.[39]
In addition to helping prevent Medicaid cuts, additional FMAP increases would free up state funds that could help avert cuts to other health programs, as well as education and other crucial services — although states will need other federal fiscal relief as well.[40] Medicaid can also help fill some of the gaps left by cuts to state-funded behavioral health and other safety net health programs, particularly in Medicaid expansion states. States, for instance, can help more providers participate in Medicaid and add more behavioral health services to their state plans so that providers facing revenue losses will be reimbursed for their services. But without additional FMAP increases, states will likely cut these same services or cut payment rates for behavioral health providers.
Appendix: State Enrollment Data
Enrollment figures in this analysis are based on preliminary estimates from state websites, as of July 20, 2020. In certain instances, multiple Medicaid enrollment estimates may be available from a state’s website. We selected the estimate that appears to best capture total Medicaid enrollment in the state, and we are consistent in our selection within a state from month to month. Figures may not match official data that the CMS later reports for a variety of reasons, including that states revise their monthly enrollment totals as eligibility determinations are finalized or appealed, that monthly enrollment may reflect average enrollment over the month or enrollment on a particular day — e.g., the first day of the month — and that states may include Children’s Health Insurance Program (CHIP) enrollment. Unfortunately, CMS enrollment figures are available only through March. Both the state-reported and CMS data show virtually flat enrollment between February and March.
- Alaska reports total Medicaid enrollment for the last day of a given month. Enrollment is up 3.7 percent between February and June, or 8,109 people. Enrollment among Medicaid expansion adults is up 9.9 percent, or 5,278 people.[41]
- Arizona reports total Medicaid enrollment for the first day of a given month. Enrollment is up 7.5 percent between February and July, or 137,419 people. Enrollment among Medicaid expansion adults is up 14.0 percent, or 56,521 people.[42]
- Arkansas reports total Medicaid enrollment for the first day of a given month. Enrollment is up 2.8 percent between February and May, or 25,412 people. Enrollment among Medicaid expansion adults is up 4.6 percent, or 11,499 people.[43]
- Colorado reports total Medicaid enrollment for the 15th day of a given month. Enrollment is up 5.1 percent between February and May, or 60,869 people. Enrollment among Medicaid expansion adults is up 8.3 percent, or 31,092 people.[44]
- Connecticut reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 4.8 percent between February and June, or 49,259 people. Enrollment among Medicaid expansion adults is up 6.2 percent, or 16,345 people.[45]
- Florida reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 9.8 percent between February and June, or 370,242 people.[46]
- Illinois reports only managed care Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 2.2 percent between February and May, or 48,822 people. Enrollment data for We do not have data for Medicaid expansion adults.[47]
- Indiana reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 8.0 percent between February and May, or 115,336 people. Enrollment among Medicaid expansion adults is up 18.1 percent, or 78,107 people.[48]
- Iowa reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 7.1 percent between February and July, or 43,517 people. Enrollment among Medicaid expansion adults is up 9.7 percent, or 16,782 people. [49]
- Kansas reports total Medicaid enrollment for the last day of a given month. Enrollment is up 5.9 percent between February and June, or 21,275 people.[50]
- Kentucky reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 14.3 percent between February and July, or 187,844 people.[51]
- Louisiana reports enrollment among Medicaid expansion adults for the 12th day of a given month. Medicaid expansion enrollment is up 6.9 percent between February and June, or 33,312 people. We do not have data on total Medicaid enrollment.[52]
- Maine reports enrollment among Medicaid expansion adults for the first day of a given month. Medicaid expansion enrollment is up 30.5 percent between February and July, or 13,480 people. We do not have data on total Medicaid enrollment.[53]
- Maryland reports total Medicaid enrollment among Medicaid expansion adults for the last day of a given month. Enrollment is up 1.7 percent between February and May, or 23,963 people. We do not have data for Medicaid expansion adults.[54]
- Michigan reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 1.7 percent between February and April, or 29,610 people. Enrollment among Medicaid expansion adults is up 1.3 percent, or 6,827 people.[55]
- Minnesota reports only managed care Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 13.6 percent between February and July, or 123,505 people. We do not have data for Medicaid expansion adults.[56]
- Mississippi reports total Medicaid enrollment for the last day of a given month. Enrollment is up 3.9 percent between February and June, or 25,920 people.[57]
- Missouri reports only managed care Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 8.8 percent between February and May, or 75,000 people.[58]
- Montana reports enrollment among Medicaid expansion adults for the first day of a given month. Medicaid expansion enrollment is up 2.0 percent between February and June, or 1,612 people. We do not have data on total Medicaid enrollment.[59]
- New Hampshire reports total Medicaid enrollment for the last day of a given month. Enrollment is up 8.1 percent between February and June, or 14,506 people. Enrollment among Medicaid expansion adults is up 14.2 percent, or 7,344 people.[60]
- New Jersey reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 5.3 percent between February and June, or 89,432 people. Enrollment among Medicaid expansion adults is up 9.6 percent, or 58,124 people.[61]
- New Mexico reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 3.7 percent between February and June, or 30,579 people. Enrollment among Medicaid expansion adults is up 4.0 percent, or 10,605 people.[62]
- New York reports only managed care Medicaid enrollment for the first day of a given month. Enrollment is up 7.5 percent between February and June, or 314,802 people. Enrollment among Medicaid expansion adults is up 10.1 percent, or 310,384 people.[63]
- North Carolina reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 4.6 percent between February and June, or 95,078 people.[64]
- Ohio reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 7.1 percent between February and June, or 196,725 people. Enrollment among Medicaid expansion adults is up 13.3 percent, or 81,368 people.[65]
- Oklahoma reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 6.1 percent between February and May, or 47,936 people.[66]
- Oregon reports only managed care Medicaid enrollment for the 15th day of a given month. Enrollment is up 4.5 percent between February and June, or 45,135 people. EWe do not have data for Medicaid expansion adults.[67]
- South Dakota reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 0.9 percent between February and April, or 989 people.[68]
- Tennessee reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 1.9 percent between February and June, or 27,549 people.[69]
- Texas reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 3.5 percent between February and April, or 133,404 people.[70]
- Utah reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 11.6 percent between February and June, or 33,899 people. Enrollment among Medicaid expansion adults is up 24.3 percent, or 11,641 people.[71]
- Virginia reports total Medicaid enrollment for the first day of a given month. Enrollment is up 8.6 percent between February and July, or 116,133 people. Enrollment among Medicaid expansion adults is up 14.2 percent, or 54,254 people.[72]
- Washington reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 3.2 percent between February and June, or 58,595 people. Enrollment among Medicaid expansion adults is up 7.8 percent, or 43,404 people.[73]
- West Virginia reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 4.1 percent between February and June, or 20,865 people. We do not have data for Medicaid expansion adults.[74]
- Wisconsin reports total Medicaid enrollment without specifying how monthly enrollment is defined. Enrollment is up 7.9 percent between February and June, or 93,812 people.[75]
End Notes
[1] Our enrollment analysis draws upon and updates by Joan Alker and Tricia Brooks, “Medicaid Enrollment Increases Show Surprisingly Wide Variability Among States,” Georgetown Center for Children and Families, July 2, 2020, https://ccf.georgetown.edu/2020/07/02/medicaid-enrollment-increases-show-surprisingly-wide-variability-among-state/. For additional details, see the appendix.
[2] CBO’s forecast is here: https://www.cbo.gov/publication/56442. The Urban Institute analysis provides estimates for Medicaid growth assuming a 15 or 20 percent unemployment rate; we extrapolate the figures for a 10 percent unemployment rate. Bowen Garrett and Anuj Gangopadhyaya, “How the COVID-19 Recession Could Affect Health Insurance Coverage,” Urban Institute, May 2020, https://www.urban.org/sites/default/files/publication/102157/how-the-covid-19-recession-could-affect-health-insurance-coverage_0.pdf.
[3] Gia Gould, “Early Evidence Suggests Increased Medicaid Enrollment Due to COVID-19,” National Academy for State Health Policy, June 1, 2020, https://www.nashp.org/early-evidence-suggests-increased-medicaid-enrollment-due-to-covid-19/.
[4] We evaluate Medicaid, SNAP, and unemployment insurance monthly enrollment from November 2007 through December 2009. We use Centers for Medicare & Medicaid Services’ monthly Medicaid enrollment data (https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidDataSourcesGenInfo/MSIS-Tables), U.S. Department of Agriculture Food and Nutrition Service SNAP enrollment data (https://www.fns.usda.gov/pd/supplemental-nutrition-assistance-program-snap) and Department of Labor unemployment insurance claims data (https://oui.doleta.gov/unemploy/claims.asp).
[5] See also Alker and Brooks, op. cit., which our analysis draws on and updates, and Elizabeth Hinton et al., “Data Note: Growth in Medicaid MCO Enrollment During the COVID-19 Pandemic,” Kaiser Family Foundation, July 16, 2020, https://www.kff.org/coronavirus-covid-19/issue-brief/data-note-growth-in-medicaid-mco-enrollment-during-the-covid-19-pandemic/.
[6] While enrollment increases are likely driven mainly by economic conditions, the Families First Coronavirus Response Act’s requirement that states pause Medicaid terminations while they receive additional federal funding is contributing to the overall increases as well, mainly by keeping eligible people from losing coverage due to paperwork requirements and to their income fluctuations from month to month. See Judith Solomon, “Continuous Coverage Protections in Families First Act Prevent Coverage Gaps by Reducing ‘Churn,’” Center on Budget and Policy Priorities, July 16, 2020, https://www.cbpp.org/research/health/continuous-coverage-protections-in-families-first-act-prevent-coverage-gaps-by.
[7] Matt Broaddus, “Research Note: Medicaid Enrollment Decline Among Children and Adults Too Large to Be Explained by Falling Unemployment,” Center on Budget and Policy Priorities, July 17, 2019, https://www.cbpp.org/research/health/medicaid-enrollment-decline-among-adults-and-children-too-large-to-be-explained-by.
[8] These figures include Maine and Virginia (which implemented their Medicaid expansions beginning in 2019) and Utah (which fully implemented its Medicaid expansion beginning in 2020). In these states, expansion enrollment may be growing in part because it had not yet reached steady levels. All three states, however, have seen a sharp acceleration in growth rates since the recession began. And excluding these states has little effect on our findings; without them, expansion enrollment would have grown by 9.5 percent between February and June.
[9] Jessica Schubel, “States Are Leveraging Medicaid in Response to COVID-19,” Center on Budget and Policy Priorities, updated July 14, 2020, https://www.cbpp.org/research/health/states-are-leveraging-medicaid-to-respond-to-covid-19.
[10] Elizabeth McNichol and Michael Leachman, “States Continue to Face Large Shortfalls Due to COVID-19 Effects,” Center on Budget and Policy Priorities, updated July 7, 2020, https://www.cbpp.org/research/state-budget-and-tax/states-continue-to-face-large-shortfalls-due-to-covid-19-effects.
[11] Congressional Budget Office, “Preliminary Estimate of the Effects of H.R. 6201, the Families First Coronavirus Response Act,” April 2, 2020, https://www.cbo.gov/system/files/2020-04/HR6201.pdf.
[12] State of Arizona, “JLBC Staff – June Budget Update,” June 19, 2020, p. 5, https://www.azleg.gov/jlbc/061920junebudgetupdate.pdf; State of California, “California State Budget 2020-21,” p. 54, http://www.ebudget.ca.gov/FullBudgetSummary.pdf; State of Colorado, “Budget Package and Long Bill Narrative,” May 26, 2020, p. 48, https://leg.colorado.gov/sites/default/files/fy20lbnarrative.pdf; State of Georgia, “HB 793 - FY 2021 Appropriations Bill,” p. 40, https://opb.georgia.gov/hb-793-fy-2021-appropriations-bill; State of Louisiana, “Overall House Floor - Solution to SGF Shortfalls,” p. 1, https://house.louisiana.gov/housefiscal/hac/State%20Budget%20Summary%20-%20House%20Floor%20After%20HAC%205-22-20.pdf; State of Nevada, “Nevada COVID-19 Fiscal Report,” July 6, 2020, p. 24, http://gov.nv.gov/uploadedFiles/govnewnvgov/Content/News/Press/2020_attachments/Nevada_COVID-19_Fiscal_Report.pdf; State of Utah, “Medicaid and CHIP Caseload, Inflation and Program Changes,” https://cobi.utah.gov/2020/1/issues/15239.
[13] Health Access California, “2020 Budget Scorecard,” June 23, 2020, https://health-access.org/wp-content/uploads/2020/06/Health-Access-2020-Budget-Scorecard_6.23.20.pdf.
[14] Governor Gavin Newsom, Letter to Senate Majority Leader Mitch McConnell and Minority Leader Chuck Schumer, June 26, 2020, https://drive.google.com/file/d/1-83dGWGRSvd7F3cXZ2z_4rm_SCgikMMb/view?usp=sharing
[15] Colorado Consumer Health Initiative, “2020 Legislative Summary,” https://cohealthinitiative.org/wp-content/uploads/2020/06/2020-Legislative-Scorecard_FINAL_6.24.20-reduced-size.pdf. See also Markian Hawryluk, “Colorado, Like Other States, Trims Health Programs Amid Health Crisis,” Kaiser Health News, July 10, 2020, https://khn.org/news/colorado-like-other-states-trims-health-programs-amid-health-crisis/.
[16] Governor Ron DeSantis, “2020 Veto List,” June 29, 2020, https://www.flgov.com/2020/06/29/governor-ron-desantis-signs-the-fiscal-year-2020-2021-budget/. See Line Item 249 for vetoes of three line items regarding provider rate increases. See also Carl Lisciandrello and Mark Schreiner, “Gov. DeSantis Vetoes $1 Billion From Florida Budget, Citing ‘Difficult Circumstances,’” News Service of Florida, June 29, 2020, https://wusfnews.wusf.usf.edu/post/gov-desantis-vetoes-1-billion-florida-budget-citing-difficult-circumstances.
[17] Nevada Assembly Bill 3, July 18, 2020, https://www.leg.state.nv.us/App/NELIS/REL/31st2020Special/Bill/7127/Text.
[18] State of Utah, “Compendium of Budget Information,” https://cobi.utah.gov/2020/1/issues.
[19] State of Tennessee, “Conference Committee Report on House Bill No. 2922 / Senate Bill No. 2931 / CC0023,” http://www.capitol.tn.gov/Bills/111/CCRReports/CC0023.pdf. See also Shannon Smith, “TennCare postpartum care expansion cut from revised state budget,” WBIR, June 8, 2020, https://www.wbir.com/article/life/tenncare-postpartum-care-expansion-cut-from-revised-state-budget/51-8587612b-7c73-4566-b5e2-be7f524ace0d.
[20] Office of Financial Management, “Budget Savings Options 2020 – Health Care Authority,” State of Washington, https://ofm.wa.gov/sites/default/files/public/budget/statebudget/savings/107HCA-HBE.pdf.
[21] Nevada Assembly Bill 3, July 18, 2020, https://www.leg.state.nv.us/App/NELIS/REL/31st2020Special/Bill/7127/Text.
[22] Wes Ventiecher, “California’s largest state worker union accepts two furlough days in pay cut deal with Newsom,” Sacramento Bee, June 20, 2020, https://www.sacbee.com/news/politics-government/the-state-worker/article243680447.html.
[23] Stacey Barchenger and Dustin Racioppi, “Gov. Murphy signs revamped bill to furlough workers as CARES money runs out,” NorthJersey.com, July 3, 2020, https://www.northjersey.com/story/news/2020/07/03/gov-phil-murphy-signs-bill-furlough-workers-stimulus-money-runs-out-cares-act/5367424002/.
[24] Governor Jay Inslee, “Furloughs and General Wage Increases,” June 17, 2020, https://www.governor.wa.gov/sites/default/files/directive/20-08%20Furloughs%20and%20General%20Wage%20Increases%20%28tmp%29.pdf.
[25] Erin Cox, “Hogan hires former campaign manager to help solve a budget crisis,” Washington Post, July 2, 2020, https://www.washingtonpost.com/local/md-politics/hogan-hires-former-campaign-manager-the-same-week-he-pitched-cutting-employee-pay-to-solve-a-budget-crisis/2020/07/02/cea6acfc-bcab-11ea-80b9-40ece9a701dc_story.html.
[26] Dan Boyd, “State hiring freeze likely first of many budget cuts,” Albuquerque Journal, April 24, 2020, https://www.abqjournal.com/1447131/state-hiring-freeze-first-of-many-likely-budget-cuts-ex-governor-were-going-to-have-to-reduce-expenditures.html.
[27] Andrew Tobias, “DeWine Administration Announces Employee Pay Cuts to Help Fill $25 Billion Ohio Budget Hole,” Cleveland.com, updated June 2, 2020, https://www.cleveland.com/open/2020/06/dewine-administration-announces-employee-pay-cuts-to-help-fill-25-billion-ohio-budget-hole.html.
[28] Tennessee Department of Finance and Administration, “Lee Administration Releases Plan to Balance Tennessee Budget,” June 4, 2020, https://www.tn.gov/finance/news/2020/6/4/lee-administration-releases-plan-to-balance-tennessee-budget.html.
[29] Alan Suderman, “Virginia Governor Orders Hiring Freeze, Agency Heads to Look for Cuts,” NBC News, April 4, 2020, https://www.nbcwashington.com/news/local/virginia-governor-orders-hiring-freeze-agency-heads-to-look-for-cuts/2262982/.
[30] Michael Leachman, “Contrary to Arguments, States Need More Federal Relief,” Center on Budget and Policy Priorities, May 6, 2020, https://www.cbpp.org/blog/contrary-to-arguments-states-need-more-federal-relief.
[31] Aviva Aron-Dine et al., “Larger, Longer-Lasting Increases in Federal Medicaid Funding Needed to Protect Coverage,” Center on Budget and Policy Priorities, May 5, 2020, https://www.cbpp.org/research/health/larger-longer-lasting-increases-in-federal-medicaid-funding-needed-to-protect.
[32] Ted Lutterman, “The Impact of the State Fiscal Crisis on State Mental Health Systems,” NASMHPD Research Institute, March 2012, http://www.nri-inc.org/media/1102/2012-the-impact-of-the-state-fiscal-crisis-on-state-mental-health-systems-lutterman.pdf.
[33] William Wan and Heather Long, “‘Cries for Help:’ Drug Overdoses Are Soaring During the Coronavirus Pandemic,” Washington Post, June 1, 2020, https://www.washingtonpost.com/health/2020/07/01/coronavirus-drug-overdose/.
[34] Markian Hawryluk, “Colorado, Like Other States, Trims Health Programs Amid Health Crisis,” Kaiser Health News, July 10, 2020, https://khn.org/news/colorado-like-other-states-trims-health-programs-amid-health-crisis/.
[35] Governor Ron DeSantis, “2020 Veto List,” June 29, 2020, https://www.flgov.com/2020/06/29/governor-ron-desantis-signs-the-fiscal-year-2020-2021-budget/. See Line Item 376 for vetoes of 19 line items for grants for services and programs related to behavioral health, substance use, crisis intervention, and people experiencing homelessness.
[36] State of Georgia, “HB 793 - FY 2021 Appropriations Bill,” https://opb.georgia.gov/hb-793-fy-2021-appropriations-bill. See also Alex Welch, “House and Senate Approve Georgia’s FY 2021 Budget,” Georgia Budget and Policy Institute, June 26, 2020, https://gbpi.org/2021-budget-proposal-update/.
[37] State of Utah, “Compendium of Budget Information,” https://cobi.utah.gov/2020/1/issues.
[38] Office of Financial Management, “Budget Savings Options 2020 – Health Care Authority,” State of Washington, https://ofm.wa.gov/sites/default/files/public/budget/statebudget/savings/107HCA-HBE.pdf and Office of Financial Management, “Budget Savings Options 2020 – Department of Social and Health Services,” State of Washington, https://ofm.wa.gov/sites/default/files/public/budget/statebudget/savings/300DSHS.pdf.
[39] Lauren Weber et al., “Hollowed-Out Public Health System Faces More Cuts Amid Virus,” Kaiser Health News, July 1, 2020, https://khn.org/news/us-public-health-system-underfunded-under-threat-faces-more-cuts-amid-covid-pandemic/.
[40] See, for example, Michael Leachman, “To Support Education, Congress Should Provide Substantial Fiscal Relief to States and Localities,” Testimony Before the House Committee on Education and Labor, Center on Budget and Policy Priorities, June 15, 2020, https://www.cbpp.org/state-budget-and-tax/to-support-education-congress-should-provide-substantial-fiscal-relief-to.
[41] http://dhss.alaska.gov/HealthyAlaska/Pages/dashboard.aspx
[42] https://www.azahcccs.gov/Resources/Downloads/PopulationStatistics/2020/July/AHCCCSPopulationbyCategory.pdf
[43] https://humanservices.arkansas.gov/newsroom/toolkits
[44] https://www.colorado.gov/pacific/hcpf/premiums-expenditures-and-caseload-reports
[45] https://data.ct.gov/Health-and-Human-Services/DSS-Medical-Benefit-Plan-Participation-by-Month-CY/f7bp-3wsx
[46] https://ahca.myflorida.com/medicaid/Finance/data_analytics/eligibles_report/index.shtml
[47] https://www.illinois.gov/hfs/MedicalProviders/cc/Pages/TotalCCEnrollmentforAllPrograms.aspx
[48] https://www.in.gov/fssa/ompp/4881.htm
[49] https://dhs.iowa.gov/ime/about/performance-data/MC-monthly-reports
[50] https://www.kdheks.gov/hcf/medicaid_reports/default.htm
[51] https://chfs.ky.gov/agencies/dms/dafm/Pages/statistics.aspx
[52] http://www.ldh.la.gov/HealthyLaDashboard/
[53] https://www.maine.gov/dhhs/data-reports/mainecare-expansion
[54] https://md-medicaid.org/eligibility/index.cfm
[55] https://www.michigan.gov/mdhhs/0,5885,7-339-71547_4860-15064--,00.html
[56] https://www.dhs.state.mn.us/main/idcplg?IdcService=GET_DYNAMIC_CONVERSION&RevisionSelectionMethod=LatestReleased&dDocName=dhs16_141529
[57] https://medicaid.ms.gov/resources/
[58] https://dss.mo.gov/mis/clcounter/history.htm
[59] https://dphhs.mt.gov/helpplan/medicaidexpansiondashboard
[60] https://www.dhhs.nh.gov/ombp/medicaid/enrollment-data.htm
[61] https://www.state.nj.us/humanservices/dmahs/news/reports/
[62] https://www.hsd.state.nm.us/LookingForInformation/medicaid-eligibility.aspx
[63] https://www.health.ny.gov/health_care/managed_care/reports/enrollment/monthly/
[64] https://medicaid.ncdhhs.gov/reports/dashboards
[65] https://medicaid.ohio.gov/RESOURCES/Reports-and-Research/Caseload-Reports
[66] http://www.okhca.org/research.aspx?id=17502
[67] https://www.oregon.gov/oha/HSD/OHP/Pages/Reports.aspx?wp2504=p:1#g_c0f44780_17ac_4f72_ab1b_ae94d4742b9e
[68] https://dss.sd.gov/keyresources/medasst_statistics.aspx
[69] https://www.tn.gov/tenncare/information-statistics/enrollment-data.html
[70] https://hhs.texas.gov/about-hhs/records-statistics/data-statistics/healthcare-statistics
[71] State health agency data as of July 10, 2020.
[72] https://www.dmas.virginia.gov/#/deidentifiedreports
[73] https://www.hca.wa.gov/about-hca/client-eligibility-data-dashboard
[74] https://dhhr.wv.gov/bms/Members/Managed%20Care/MCOreports/Pages/default.aspx
More from the Authors

Areas of Expertise

Areas of Expertise
