Frequently Asked Questions About Medicaid
Recent proposals at the federal and state levels to radically restructure Medicaid raise questions about how the program works and its current role for states, beneficiaries, and health care providers and plans. This report addresses some of these questions.[1]
How Efficient Is Medicaid?
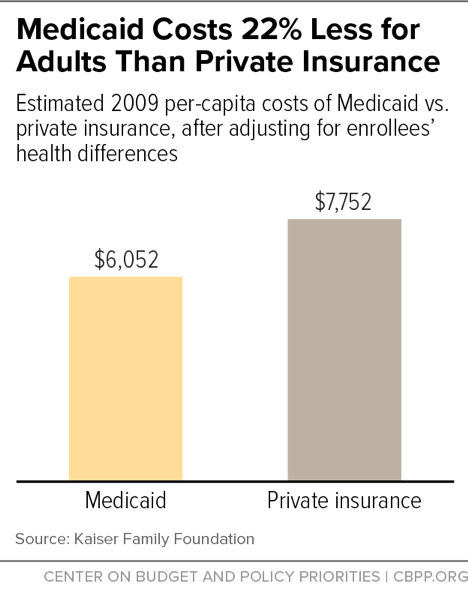
Medicaid’s costs per beneficiary are substantially lower than for private insurance and have been growing more slowly than per-beneficiary costs under private employer coverage.
Medicaid provides more comprehensive benefits than private insurance at significantly lower out-of-pocket cost to beneficiaries, but its lower payment rates to health care providers and lower administrative costs make the program very efficient. It costs Medicaid much less than private insurance to cover people of similar health status. For example, adults on Medicaid cost about 22 percent less than if they were covered by private insurance, Urban Institute research shows.[2]
Over the past 30 years, Medicaid costs per beneficiary have essentially tracked costs in the health care system as a whole, public and private. In fact, costs per beneficiary grew more slowly for Medicaid than for private insurance between 1987 and 2017, and are expected to continue growing more slowly than for private insurance in coming years, according to the Medicaid and CHIP Payment and Access Commission.[3]
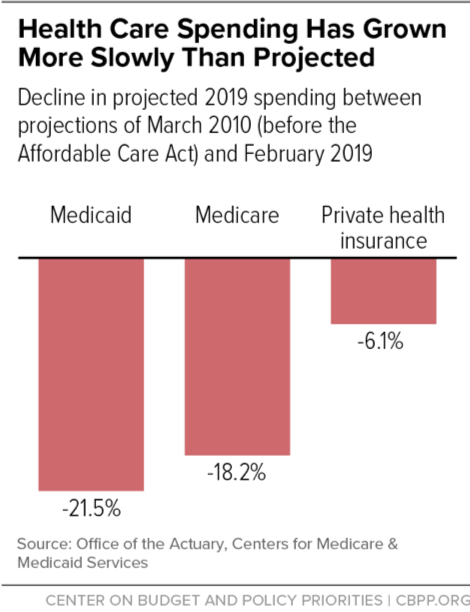
Moreover, the Centers for Medicare & Medicaid Services (CMS), which projected in 2010 — before enactment of the Affordable Care Act (ACA) — that Medicaid spending would total $794 billion by 2019, has lowered its projection for 2019 by 21.5 percent to $623 billion, even with the ACA’s coverage expansions. (See Figure 2.)
How Much Flexibility Do States Have to Design Their Own Programs?
Medicaid gives states expansive flexibility to design their own programs — whom they cover, what benefits they provide, and how they deliver health care services.
The federal government sets minimum standards, including specifying certain categories of people that all states must cover and certain health coverage they must provide. Beyond that, states are free to set their own rules. For example, states have broad flexibility to decide which “optional” categories of low-income people to cover, and up to what income levels. As a result, Medicaid eligibility varies substantially from state to state.
Medicaid benefit packages vary significantly by state as well. States have flexibility to determine whether to cover services like dental and vision care for adults and can determine the amount, duration, and scope of the services they provide.
States also have flexibility over how they deliver health care services. Many states rely heavily on managed care plans to deliver care, while others use provider-sponsored organizations, health homes, and accountable care organizations (groups of providers and other entities that partner to provide a range of health care services in a coordinated way).[4]
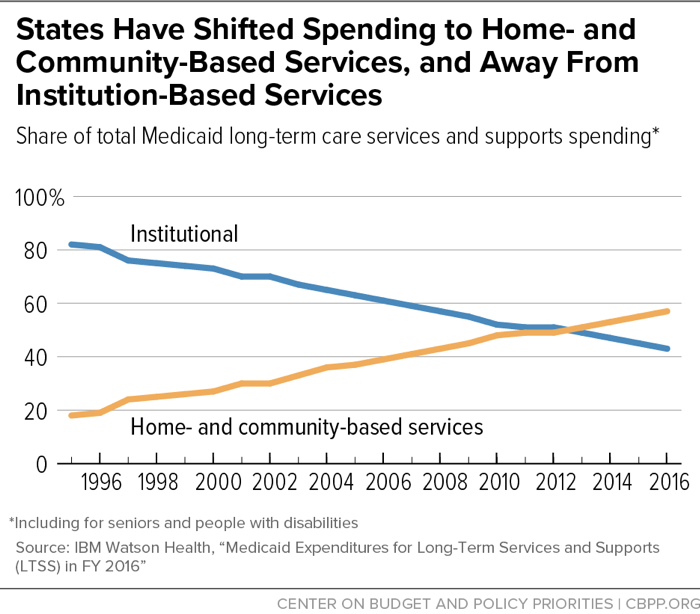
Medicaid is the primary payer for long-term services and supports, including nursing home care and home health services, the need for which is expected to grow considerably as the population ages.[5] Using Medicaid’s flexibility — including a number of new state options created by the ACA — states have greatly expanded home- and community-based services (HCBS) so more people with long-term service and support needs can stay in their homes and communities rather than move to nursing homes and other institutions. The share of Medicaid spending on long-term services and supports going to HCBS rose from 18 percent to 57 percent between 1995 and 2016.[6] (See Figure 3.)
States have taken advantage of Medicaid’s flexibility in other ways to improve beneficiary health outcomes while lowering costs.[7] For example, states are employing strategies to improve the delivery of care, particularly for beneficiaries with chronic conditions who use the most care.[8] For example, a Wisconsin hospital is testing a new way to integrate health services for Medicaid-eligible children with complex medical needs, a rapidly growing group with high health care costs.[9] An early evaluation of Wisconsin’s model showed that inpatient hospital days and costs fell by more than 50 percent after children enrolled in the program.[10]
Similarly, Oregon has established, through a Medicaid waiver, a network of accountable care organizations to integrate hospital-based services with primary care, behavioral health care, and other social supports.[11] Oregon has seen emergency department visits and preventable hospital admissions fall significantly, while lowering its growth in Medicaid spending per beneficiary by two percentage points below the levels projected without the waiver.[12]
Do Beneficiaries Have Adequate Access to Health Care?
Numerous studies show that Medicaid helps make millions of Americans healthier by improving access to preventive and primary care and by protecting against (and providing care for) serious diseases.
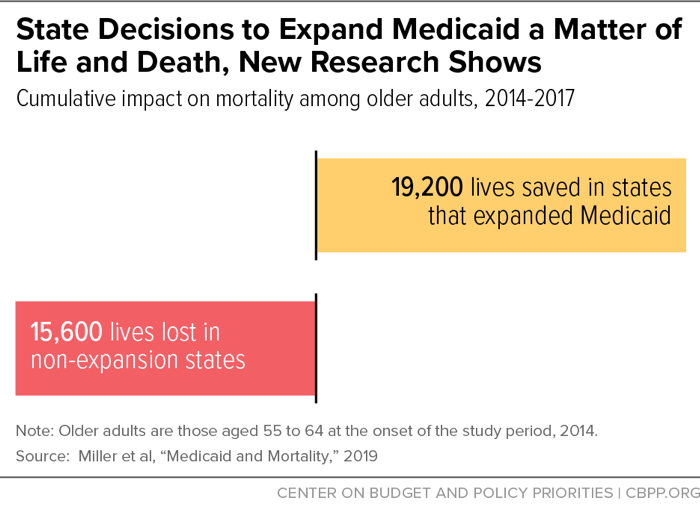
Notably, the ACA’s expansion of Medicaid to low-income adults prevents thousands of premature deaths each year, a landmark study found.[13] It saved the lives of at least 19,200 adults aged 55 to 64 over the four-year period from 2014 to 2017. Conversely, 15,600 older adults died prematurely because of some states’ decisions not to expand Medicaid. (See Figure 4.) The lifesaving impacts of Medicaid expansion are large: an estimated 39 to 64 percent reduction in annual mortality rates for older adults gaining coverage.[14]
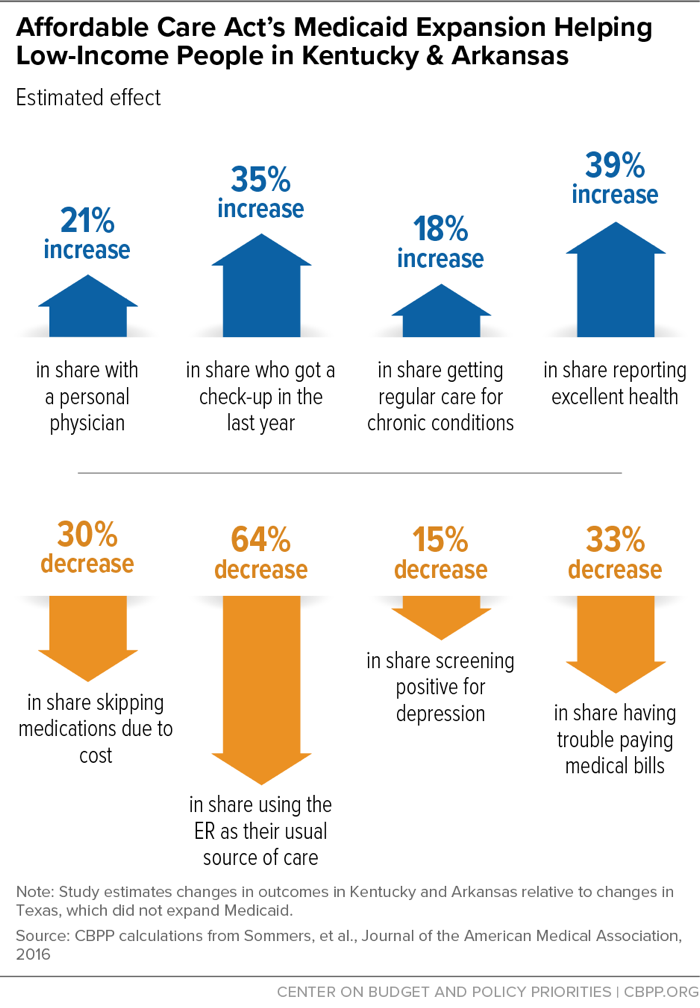
This new research is consistent with earlier studies finding that the ACA’s Medicaid expansion improves the health and financial well-being of those who newly gain coverage.[15] One recent study, for example, found that expansion states had a lower mortality rate for near-elderly adults than non-expansion states.[16] Another study, comparing low-income adults in Arkansas and Kentucky (which adopted the expansion) with similar adults in Texas (which has not expanded), found the expansion has increased utilization of primary care and screenings and treatment for chronic conditions like diabetes. It has also resulted in fewer skipped medications due to cost, lower out-of-pocket medical spending, and improved overall health. (See Figure 5.) Moreover, the benefits of the Medicaid expansion grew in its second year of implementation, the study found.[17]
Another important study, of Oregon’s pre-ACA Medicaid expansion, found that people with Medicaid were 40 percent less likely than similar people without coverage to have suffered a decline in their health in the previous six months.[18] They were also more likely to use preventive care (such as cholesterol screenings), to have a regular office or clinic where they could receive primary care, and to receive diagnosis of and treatment for depression and diabetes.[19] And they were 40 percent less likely than those without insurance to go into medical debt or leave other bills unpaid in order to cover medical expenses. In fact, the latest research from Oregon found that Medicaid coverage “nearly eliminated catastrophic out-of-pocket medical expenditures.”[20]
Other pre-ACA expansions of Medicaid coverage for low-income adults, in Arizona, Maine, and New York, reduced mortality by 6.1 percent, research published in the New England Journal of Medicine reported.[21]
Urban Institute researchers also have found that Medicaid provides beneficiaries with access to health care services that is comparable to — but less costly on an out-of-pocket basis than — what they would receive through employer-sponsored insurance. If these beneficiaries were uninsured, they would be significantly less likely to have a usual source of care and more likely to forgo needed health care services.[22]
The Medicaid and CHIP Payment Access Commission also finds that access to health care is significantly better among non-elderly adult Medicaid beneficiaries than among the uninsured. Some 85 percent of non-elderly adult Medicaid beneficiaries have a regular source of care, nearly twice the figure for non-elderly adults without coverage. Similarly, Medicaid beneficiaries are much more likely to visit a primary care physician, to visit a specialist, and to have a routine check-up.[23]
Surveys have found that Medicaid enrollees are largely satisfied with their access to care. Eighty-eight percent of Medicaid enrollees reported being somewhat or very satisfied with their doctor, and 91 percent report having a regular source of care.[24] Medicaid enrollees are also less likely to have trouble paying medical bills or skip needed care due to cost than people with private coverage — even though most Medicaid beneficiaries have low incomes.[25]
Finally, obtaining access to health care through Medicaid offers long-term benefits. For example, for black children, Medicaid eligibility during early childhood reduced mortality rates in their later teenage years by 13 to 20 percent, research from University of Chicago analysts finds.[26] In addition, black individuals eligible for Medicaid for more of their childhood have fewer hospitalizations and emergency room visits as adults. And children eligible for Medicaid for more of their childhood earn more as adults and are more likely to attend and complete college.[27]
How Does Medicaid Affect Work Incentives?
Medicaid supports work, evidence shows.[28] Most Medicaid beneficiaries who can work do so: two-thirds of non-elderly adults enrolled in Medicaid who don’t receive federal disability benefits live in a family with at least one worker.[29] Moreover, one recent study found that people in states with more generous Medicaid eligibility levels and benefits are more likely to leave a job for another position with greater growth potential.[30] This research suggests that comprehensive Medicaid coverage can support work and help beneficiaries take advantage of promising job opportunities without worrying about losing their coverage.
In 2018, the Trump Administration began encouraging states to take Medicaid coverage away from people who are not working or participating in work-related activities for a specified number of hours each month.[31] In Arkansas, the first state to implement such a policy, more than 18,000 individuals lost coverage in the first seven months,[32] before a federal court blocked the policy.[33] Researchers found no significant increases in employment, number of hours worked, or overall rates of community engagement activities among those subject to the work requirement.[34]
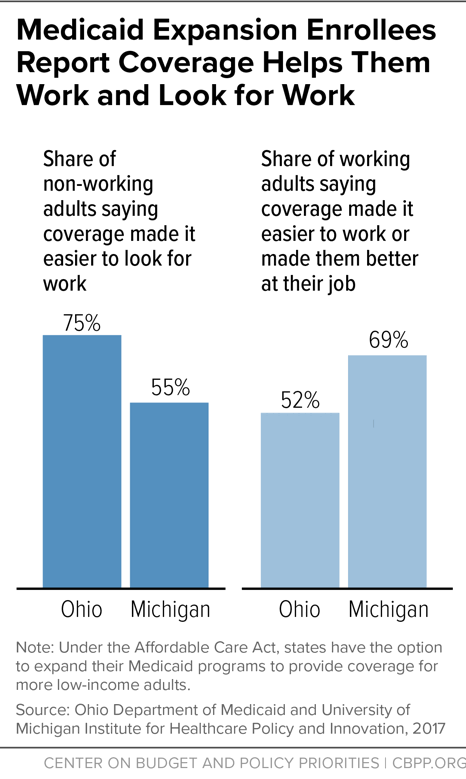
In contrast, studies conducted in Michigan and Ohio show that Medicaid expansion enrollees with jobs said Medicaid coverage made it easier for them to maintain employment, while those without jobs said coverage made it easier for them to look for employment.[35] (See Figure 6.) “[N]o studies have found negative effects of expansion” on employment or employee behavior, according to a comprehensive literature review by the Kaiser Family Foundation.[36]
In fact, the Medicaid expansion significantly reduces work disincentives among working-poor parents. Before it took effect in 2014, Medicaid eligibility for working parents cut off at just 61 percent of the poverty line in the typical state, or roughly $13,000 for a family of three in 2019.[37] As a result, a poor parent would lose Medicaid if she worked more hours or took a higher-paying job, though her children would still be eligible for Medicaid or the Children’s Health Insurance Program (CHIP). She could receive transitional Medicaid for a limited time but would likely end up uninsured if her employer didn’t offer job-based coverage (most very low-wage jobs don’t come with health coverage) or she couldn’t afford it.
Now, in the 33 states and the District of Columbia that have expanded Medicaid under the ACA, the Medicaid eligibility limit for working parents is 138 percent of the poverty line, about $17,200 for an individual and $29,400 for a family of three in 2019. If a family’s income rises above this level, the working parent can get subsidized coverage through the health insurance marketplaces.
Thus, the Medicaid expansion enables tens of millions of working parents to seek higher wages or to work more hours without forgoing health coverage. As a Congressional Budget Office report states, “some people who would have been eligible for Medicaid under prior law — in particular, working parents with very low income — will work more” due to the expansion.[38]
Two recent studies comparing changes in the labor market participation of low-income adults in expansion and non-expansion states show that the expansion has not reduced work among those newly eligible. One found that low-income workers in expansion states did not lose jobs, switch jobs, or change from full- to part-time work more frequently than low-income workers in non-expansion states.[39] The other found that the Medicaid expansion did not meaningfully affect the incidence of job loss, number of hours usually worked, or probability of working more than 30 hours.[40]
How Does the ACA’s Medicaid Expansion Affect State Budgets?
Under the ACA, the federal government paid 100 percent of the cost of Medicaid expansion coverage from 2014 to 2016. The federal share then dropped gradually to 93 percent in 2019 and will settle at 90 percent in 2020 and each year thereafter. By comparison, the federal government pays between 50 and 76 percent of the cost of other Medicaid enrollees, depending on the state.
Many states and independent analyses have found that the Medicaid expansion has not only helped more than 12 million low-income people gain health coverage but also produced net savings for state budgets.[41] It has done so by allowing states to move people who previously received health services through targeted Medicaid programs financed at the state’s regular match rate, such as family-planning services and care for certain women with breast and cervical cancer, into the new expansion group, for which the federal government pays nearly all of the cost. And as more low-income uninsured residents have gained coverage, demand for entirely state-funded services that serve the uninsured has declined, such as funding for hospitals’ uncompensated care costs and for mental health services. States like Arkansas, Colorado, Michigan, and Virginia expect the expansion to produce net budgetary savings in the coming years even though states have had to pay a modest share of the expansion costs since 2017.
Despite this evidence, critics of Medicaid expansion have claimed that expansion has financially harmed states because some states underestimated the number of people who would enroll. This argument doesn’t hold up under scrutiny. As a review of studies on the cost of expansion concluded, “[c]laims that the costs of Medicaid expansion have far exceeded expectations are overstated, misleading, and substantially inaccurate, based on a review of the credible evidence from either academic or government sources.”[42]
Does Medicaid Primarily Cover People Who Otherwise Would Have Private Coverage?
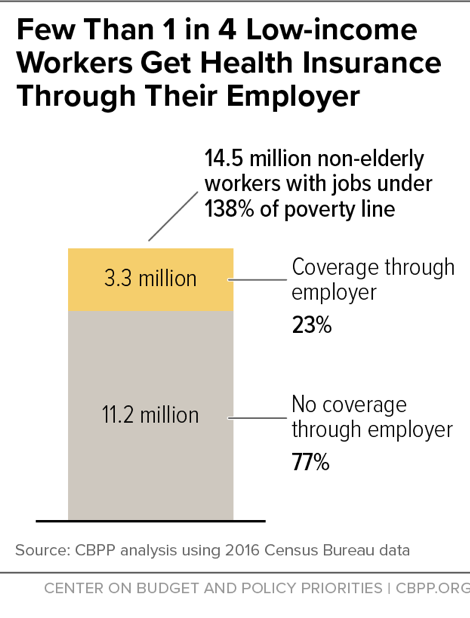
The overwhelming majority of people who get coverage under the ACA’s Medicaid expansion are low-income individuals who would otherwise be uninsured. Many work in low-wage jobs for small firms or service industries that typically don’t offer health insurance. And unsubsidized coverage in the individual insurance market would be unaffordable for most of those eligible for the Medicaid expansion.
- Some 79 percent of workers earning less than 138 percent of the poverty line — the limit to qualify for Medicaid under the expansion — do not get coverage through their employer. (See Figure 7.)
- The median annual cost of single coverage in the pre-ACA individual market, including premiums and out-of-pocket costs, would have consumed more than one-third of the total income of a family of three at the poverty line, making such coverage essentially unaffordable.
A study by Urban Institute researchers finds that from 2013 to 2017 (as expansion took effect), the share of non-elderly low-income workers with Medicaid or other public coverage increased by 20.5 percentage points in expansion states, while the share with employer-sponsored coverage remained unchanged. The uninsured rate fell by 22.7 percentage points, reflecting the large increase in Medicaid coverage and a small increase in the share with individual market coverage, presumably through the ACA marketplaces. The study also finds no change in employers offering coverage to low-income workers.[43]
What Share of Eligible People Participate in Medicaid?
Medicaid participation is quite high, particularly among children in states that have made concerted efforts to simplify and streamline their enrollment processes. For example, prior to the Medicaid expansion, some 68 percent of low-income adults with children who are eligible for Medicaid were enrolled, according to the Urban Institute,[44] a relatively strong rate compared to some other programs.[45] And 12.4 million low-income adults newly eligible under the Medicaid expansion had enrolled by the third quarter of 2017, along with another 4.6 million individuals who were previously eligible but unenrolled and enrolled due to the Medicaid expansion.[46]
In addition, nearly 94 percent of eligible children participated in Medicaid or CHIP in 2016, according to the Urban Institute.[47] That is an exceedingly high rate for a means-tested program; in a number of states, children’s Medicaid participation matches or exceeds the participation rates for universal social insurance programs like Medicare Part B.[48] Since CHIP’s enactment in 1997, states have taken a number of steps to boost Medicaid and CHIP enrollment among eligible children, such as streamlining application procedures. The ACA requires states to take additional steps to increase the percentage of eligible children enrolling.
Focus groups with low-income, uninsured adults that the Kaiser Family Foundation conducted also bear on this issue. They found no evidence that Medicaid carries a “stigma” that discourages eligible people from enrolling. To the contrary, adults in Nevada, Texas, Florida, and Ohio — all states with very limited Medicaid eligibility before the ACA — said they were eager to enroll in Medicaid. While they wished their financial circumstances were better, they wanted affordable coverage and often couldn’t get it from their employers. Furthermore, focus group members with previous experience with Medicaid (often because their children were eligible) spoke favorably of it as affordable and covering a broad set of services and medications.[49]
End Notes
[1] See also Matt Broaddus and Edwin Park, “Ryan Poverty Report’s Criticism of Medicaid Misrepresents Research Literature,” Center on Budget and Policy Priorities, March 31, 2014, https://www.cbpp.org/cms/index.cfm?fa=view&id=4114.
[2] Teresa Coughlin et al., “What Difference Does Medicaid Make? Assessing Cost-Effectiveness, Access and Financial Protection under Medicaid for Low-Income Adults,” Kaiser Family Foundation, May 3, 2013, http://kff.org/medicaid/issue-brief/what-difference-does-medicaid-make-assessing-cost-effectiveness-access-and-financial-protection-under-medicaid-for-low-income-adults/.
[3] Medicaid and CHIP Payment and Access Commission, “Report to Congress on Medicaid and CHIP,” June 2016, https://www.macpac.gov/wp-content/uploads/2016/06/Trends-in-Medicaid-Spending.pdf.
[4] Kaiser Family Foundation, “Medicaid Delivery System and Payment Reform: A Guide to Key Terms and Concepts,” June 2015, http://kff.org/medicaid/fact-sheet/medicaid-delivery-system-and-payment-reform-a-guide-to-key-terms-and-concepts/.
[5] Erica L. Reaves and MaryBeth Musumeci, “Medicaid and Long-Term Services and Supports: A Primer,” Kaiser Family Foundation, December 15, 2015, http://kff.org/medicaid/report/medicaid-and-long-term-services-and-supports-a-primer/.
[6] Steve Eiken et al., “Medicaid Expenditures for Long-Term Services and Supports (LTSS) in FY 2016,” Truven Health Analytics, May 2018, https://www.medicaid.gov/medicaid/ltss/downloads/reports-and-evaluations/ltssexpenditures2016.pdf.
[7] Hannah Katch, “States are Using Flexibility to Create Successful, Innovative Medicaid Programs,” Center on Budget and Policy Priorities, June 13, 2016, https://www.cbpp.org/research/health/states-are-using-flexibility-to-create-successful-innovative-medicaid-programs.
[8] Centers for Medicare & Medicaid Services, “Targeting Medicaid Super-Utilizers to Decrease Costs and Improve Quality,” CMCS Information Bulletin, July 24, 2013, http://www.medicaid.gov/federal-policy-guidance/downloads/CIB-07-24-2013.pdf.
[9] Center for Medicare and Medicaid Innovation, “Health Care Innovation Awards Round Two Project Profiles,” July 2014, https://innovation.cms.gov/Files/x/HCIATwoPrjProCombined.pdf.
[10] Christine Schindler, “Complex Care Medical Services: Inpatient Outpatient, and Homecare Focused Patient Management Model,” presentation at 38th National Conference on Pediatric Health Care, March 2017, https://www.melnic.com/wp-content/uploads/2018/09/Advanced-Practice-Provider-Complex-Care-Models-and-Roles.pdf; John B. Gordon et al., “A Tertiary Care-Primary Care Partnership Model for Medically Complex and Fragile Children and Youth with Special Health Care Needs,” JAMA Pediatrics, October 2007.
[11] State of Oregon, 1115 Waiver Demonstration Renewal, https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/or/Health-Plan/or-health-plan2-ext-appvl-01122017.pdf.
[12] Sarah Klein, Douglas McCarthy, and Alexander Cohen, “Health Share of Oregon: A Community-Oriented Approach to Accountable Care for Medicaid Beneficiaries,” Commonwealth Fund, October 2014, http://www.commonwealthfund.org/~/media/files/publications/case-study/2014/oct/1769_klein_hlt_share_oregon_aco_case_study.pdf.
[13] Sarah Miller et al., “Medicaid and Mortality: New Evidence from Linked Survey and Administrative Data,” National Bureau of Economic Research Working Paper 26081, August 2019, https://www.nber.org/papers/w26081.
[14] Matt Broaddus and Aviva Aron-Dine, “Medicaid Expansion Has Saved At Least 19,000 Lives, New Research Finds,” Center on Budget and Policy Priorities, November 6, 2019, https://www.cbpp.org/research/health/medicaid-expansion-has-saved-at-least-19000-lives-new-research-finds.
[15] Larisa Antonisse et al., “The Effects of Medicaid Expansion under the ACA: Updated Findings from a Literature Review,” Kaiser Family Foundation, March 28, 2018, https://www.kff.org/medicaid/issue-brief/the-effects-of-medicaid-expansion-under-the-aca-updated-findings-from-a-literature-review-march-2018/.
[16] Miller et al., op. cit.
[17] Benjamin Sommers et al., “Changes in Utilization and Health Among Low-Income Adults After Medicaid Expansion or Expanded Private Insurance,” JAMA Internal Medicine, August 8, 2016, http://archinte.jamanetwork.com/article.aspx?articleid=2542420.
[18] Amy Finkelstein et al., “The Oregon Health Insurance Experiment: Evidence from the First Year,” National Bureau of Economic Research Working Paper 17190, July 2011, http://www.nber.org/papers/w17190. See also Judith Solomon, “Does Medicaid Matter? New Study Shows How Much,” Center on Budget and Policy Priorities, July 7, 2011, https://www.cbpp.org/blog/does-medicaid-matter-new-study-shows-how-much.
[19] Katherine Baicker et al., “The Oregon Experiment — Effects of Medicaid on Clinical Outcomes,” New England Journal of Medicine, May 2, 2013, 368:1713-1722.
[20] Baicker et al., op. cit.
[21] Benjamin Sommers, Katherine Baicker, and Arnold Epstein, “Mortality and Access to Care among Adults after State Medicaid Expansions,” New England Journal of Medicine, September 13, 2012, 367:1025-1034.
[22] Coughlin et al., op. cit.
[23] “MACStats: Medicaid and CHIP Data Book,” Medicaid and CHIP Payment and Access Commission, December 2016, https://www.macpac.gov/wp-content/uploads/2016/12/MACStats_DataBook_Dec2016.pdf. See also David Blumenthal et al., “Does Medicaid Make a Difference? Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2014,” Commonwealth Fund, June 2015, http://www.commonwealthfund.org/~/media/files/publications/issue-brief/2015/jun/1825_blumenthal_does_medicaid_make_a_difference_ib_v2.pdf.
[24] Munira Z. Gunja et al., “How Medicaid Enrollees Fare Compared with Privately Insured and Uninsured Adults,” Commonwealth Fund, April 2017, https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_2017_apr_gunja_how_medicaid_enrollees_fare_ib.pdf.
[25] Ibid.
[26] Bruce Meyer and Laura Wherry, “Saving Teens: Using a Policy Discontinuity to Estimate the Effects of Medicaid Eligibility,” National Bureau of Economic Research Working Paper 18309, August 2012, http://www.nber.org/papers/w18309.pdf.
[27] Matt Broaddus, “Medicaid’s Long-Term Earnings and Health Benefits,” Center on Budget and Policy Priorities, May 12, 2015, https://www.cbpp.org/blog/medicaids-long-term-earnings-and-health-benefits. See also Sarah Cohodes et al., “The Effect of Child Health Insurance Access on Schooling: Evidence from Public Insurance Expansions,” National Bureau of Economic Research Working Paper 20178, May 2014, http://www.nber.org/papers/w20178.pdf.
[28] Hannah Katch, Jennifer Wagner, and Aviva Aron-Dine, “Taking Medicaid Coverage Away From People Not Meeting Work Requirements Will Reduce Low-Income Families’ Access to Care and Worsen Health Outcomes,” Center on Budget and Policy Priorities, August 13, 2018, https://www.cbpp.org/research/health/taking-medicaid-coverage-away-from-people-not-meeting-work-requirements-will-reduce.
[29] Rachel Garfield et al., “Understanding the Intersection of Medicaid and Work: What Does the Data Say?” Kaiser Family Foundation, August 8, 2019, https://www.kff.org/medicaid/issue-brief/understanding-the-intersection-of-medicaid-and-work-what-does-the-data-say/.
[30] Ammar Farooq and Adriana Kugler, “Beyond Job Lock: Impacts of Public Health Insurance on Occupational and Industrial Mobility,” NBER, March 2016, https://www.nber.org/papers/w22118.pdf.
[31] For more information on the effects of taking coverage away from people who don’t meet work requirements, see Jennifer Wagner and Judith Solomon, “States’ Complex Medicaid Waivers Will Create Costly Bureaucracy and Harm Eligible Beneficiaries,” Center on Budget and Policy Priorities, May 23, 2018, https://www.cbpp.org/research/health/states-complex-medicaid-waivers-will-create-costly-bureaucracy-and-harm-eligible; Hannah Katch, Jennifer Wagner, and Aviva Aron-Dine, “Taking Medicaid Coverage Away From People Not Meeting Work Requirements Will Reduce Low-Income Families’ Access to Care and Worsen Health Outcomes,” Center on Budget and Policy Priorities, updated August 13, 2018, https://www.cbpp.org/research/health/taking-medicaid-coverage-away-from-people-not-meeting-work-requirements-will-reduce; and Jennifer Wagner and Jessica Schubel, “States’ Experiences Confirming Harmful Effects of Medicaid Work Requirements,” Center on Budget and Policy Priorities, updated October 22, 2019, https://www.cbpp.org/sites/default/files/atoms/files/12-18-18health.pdf.
[32] Benjamin Sommers et al., “Medicaid Work Requirements — Results from the First Year in Arkansas,” New England Journal of Medicine, June 2019, https://www.nejm.org/doi/full/10.1056/NEJMsr1901772.
[33] National Health Law Program, “Federal Court Rules Against Trump Administration’s Kentucky and Arkansas Medicaid Waiver Projects That Include Work Requirements,” March 27, 2019, https://healthlaw.org/news/federal-court-rules-against-trump-administrations-kentucky-and-arkansas-medicaid-waiver-projects-that-include-work-requirements/.
[34] Sommers 2019, op cit.
[35] Ohio Department of Medicaid, “Ohio Medicaid Group VIII Assessment: A Report to the Ohio General Assembly,” January 2017, http://medicaid.ohio.gov/Portals/0/Resources/Reports/Annual/Group-VIII-Assessment.pdf. See also Kara Gavin, “Medicaid Expansion Helped Enrollees Do Better at Work or in Job Searches,” University of Michigan Health Lab, June 27, 2017, http://labblog.uofmhealth.org/industry-dx/medicaid-expansion-helped-enrollees-do-better-at-work-or-job-searches.
[36] Larisa Antonisse et al., “The Effects of Medicaid Expansion under the ACA: Updated Findings from a Literature Review,” Kaiser Family Foundation, August 2019, http://files.kff.org/attachment/Issue-brief-The-Effects-of-Medicaid-Expansion-under-the-ACA-Findings-from-a-Literature-Review.
[37] Martha Heberlein et al., “Getting Into Gear for 2014: Findings from a 50-State Survey of Eligibility, Enrollment, Renewal, and Cost-Sharing Policies in Medicaid and CHIP, 2012-2013,” Kaiser Family Foundation, January 2013, https://www.kff.org/medicaid/report/getting-into-gear-for-2014-findings-from-a-50-state-survey-of-eligibility-enrollment-renewal-and-cost-sharing-policies-in-medicaid-and-chip-2012-2013/.
[38] Congressional Budget Office, “Labor Market Effects of the Affordable Care Act: Updated Estimates,” February 2014, http://cbo.gov/sites/default/files/cbofiles/attachments/45010-breakout-AppendixC.pdf.
[39] Angshuman Gooptu et al., “Medicaid Expansion Did Not Result In Significant Employment Changes Or Job Reductions In 2014,” Health Affairs, Vol. 35, No.1, January 2016, http://content.healthaffairs.org/content/35/1/111.full.html.
[40] Robert Kaestner et al., “Effects of ACA Medicaid Expansions on Health Insurance Coverage and Labor Supply,” National Bureau of Economic Research Working Paper 21836, December 2015, http://www.nber.org/papers/w21836.
[41] Jesse Cross-Call, “Medicaid Expansion Continues to Benefit State Budgets, Contrary to Critics’ Claims,” Center on Budget and Policy Priorities, October 9, 2018, https://www.cbpp.org/health/medicaid-expansion-continues-to-benefit-state-budgets-contrary-to-critics-claims.
[42] Mark Hall, “Do states regret expanding Medicaid?” Brookings Institution, March 26, 2018, https://www.brookings.edu/blog/usc-brookings-schaeffer-on-health-policy/2018/03/26/do-states-regret-expanding-medicaid/.
[43] Adele Shartzer, Fredric Blavin, and John Holahan, “Employer-Sponsored Insurance Stable For Low-Income Workers In Medicaid Expansion States,” Health Affairs, Vol. 37, No. 4, April 2018, https://www.healthaffairs.org/doi/10.1377/hlthaff.2017.1205.
[44] Jennifer Haley et al., “Uninsurance and Medicaid/CHIP Participation among Children and Parents,” Urban Institute, September 2018, https://www.urban.org/sites/default/files/publication/99058/uninsurance_and_medicaidchip_participation_among_children_and_parents_updated_1.pdf.
[45] Government Accountability Office, “Means-Tested Programs: Information on Program Access Can Be an Important Management Tool,” March 2005, http://www.gao.gov/assets/250/245577.pdf.
[46] Centers for Medicare & Medicaid Services, Total Medicaid Enrollees – VIII Group Break Out Report, 2017, 3Q, August 2018, https://data.medicaid.gov/Enrollment/2017-3Q-Medicaid-MBES-Enrollment/rxbg-jqed..
[47] Haley et al., op. cit.
[48] Dahlia Remler and Sherry Glied, “What Other Programs Can Teach Us: Improving Participation in Health Insurance Programs,” American Journal of Public Health, January 2003, http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.93.1.67.
[49] Kaiser Family Foundation, “Faces of the Medicaid Expansion: Experiences of Uninsured Adults Who Could Gain Coverage,” November 2012, https://www.kff.org/health-reform/issue-brief/faces-of-the-medicaid-expansion-experiences-and/.
More from the Authors

Areas of Expertise

Areas of Expertise
