Closing the Coverage Gap Would Improve Black Maternal Health
Policymakers are paying long-overdue attention to reducing high and increasing rates of deaths and severe health complications among Black people who give birth. Comprehensively addressing this challenge and the broader maternal health crisis requires making a continuum of high-quality health coverage, health care, and other services accessible before, during, and after pregnancy. But the Medicaid “coverage gap” — in which adults with low incomes have no pathway to affordable coverage because their state is one of 12 that has refused to expand Medicaid — puts continuous health coverage out of reach for over 800,000 women of reproductive age. Federal policymakers should close the coverage gap in forthcoming recovery legislation so all women of reproductive age with incomes below the poverty line can get affordable coverage whether they are pregnant or not.
"Among developed countries, the United States has the highest rate of people dying of pregnancy-related complications during or within 12 months of the end of pregnancy."Among developed countries, the United States has the highest rate of people dying of pregnancy-related complications during or within 12 months of the end of pregnancy. And it is getting worse; that rate is higher than it was 25 years ago. Black women are dying at significantly higher rates than other groups, which is linked to factors including structural racism in health care delivery and toxic stress from people’s lived experiences of racism. Black women are also twice as likely to experience severe maternal morbidity: unexpected outcomes of labor and delivery resulting in significant health consequences.
Medicaid pays for more than 40 percent of U.S. births and 65 percent of births to Black mothers, so expanding and enhancing Medicaid coverage must be part of a comprehensive strategy to address the Black maternal health crisis. States that expanded Medicaid under the Affordable Care Act have seen a significant rise in health coverage among women of reproductive age. This has improved their access to preconception and prenatal services that make pregnancy and birth safer for parent and baby. Research also shows Medicaid expansion is associated with reduced rates of maternal death, particularly for Black women.
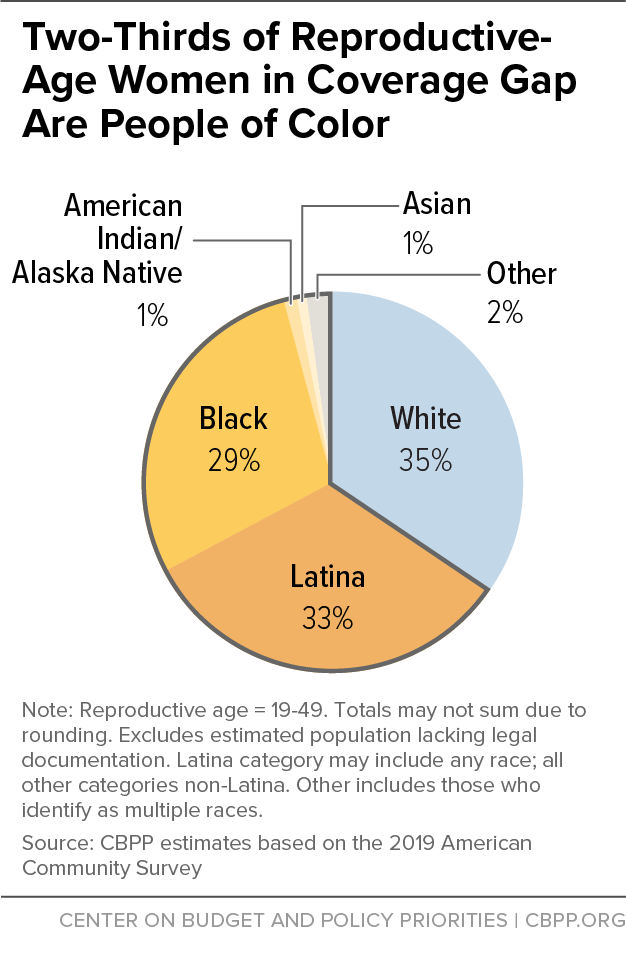
The picture is starkly different in the 12 states that have not expanded Medicaid to cover adults with incomes below 138 percent of the poverty line, or about $17,800 yearly for a single adult. These states have significantly higher uninsured rates for women of reproductive age than do expansion states. In 2019, 810,000 women of reproductive age with incomes below the poverty line — 29 percent are Black and 33 percent Latina — were uninsured without any pathway to affordable health coverage. (See Figure 1.) Almost all lived in the South, where states generally have not expanded Medicaid. (See Appendix Table 1.)
If people in the coverage gap become pregnant, they become eligible for Medicaid. But necessary preconception care is likely unavailable and being uninsured before pregnancy is associated with a higher prevalence of risk factors that contribute to poor pregnancy outcomes, especially for Black women. Moreover, uninsured people may delay prenatal care until they apply for and enroll in Medicaid.
Closing the Medicaid coverage gap is by no means sufficient to address the maternal health crisis. All states should take up the American Rescue Plan’s option to extend Medicaid pregnancy coverage for 12 months after the end of pregnancy instead of the 60 days required under current law. And states should enhance the benefits they provide, including coverage for doulas, who provide support during and after pregnancy. Moreover, numerous bills in the current Congress would invest in health care, nutrition, housing, and transportation and expand the workforce assisting pregnant people, including doulas. The Biden Administration’s budget for the Department of Health and Human Services includes $116 million for its “Improving Maternal Health in America” initiative. Investments like these are necessary to address the many factors behind high rates of maternal mortality and morbidity, especially among Black women.
People of Color’s Higher Maternal Mortality, Morbidity Rates Rooted in Structural Racism
A history of structural racism, defined as a “system in which public policies, institutional practices, and cultural representations work to perpetuate racial inequity,”a has created greater barriers to health for people of color than for white people. Structural racism is a major factor contributing to people of color’s higher rates of maternal mortality and morbidity, low birthweight and infant mortality, and lower life expectancy. The Medicaid coverage gap, which most heavily affects people of color, is itself evidence of structural racism.
Lasting exposure to adverse experiences, including structural racism, can create toxic stress that increases the likelihood of developing conditions linked to higher rates of maternal and infant death, like hypertension. Moreover, discrimination and implicit bias in the health care delivery system are often expressed in the dismissal of Black women’s concerns and symptoms, which helps explain poor outcomes even for black women with higher income and education.b Black women were ten times more likely to say they were treated unfairly than white women, a survey of women in California showed.c
Structural racism also contributes to income and wealth inequality, which manifests in unequal access to food, transportation, clean air and water, and high-quality education. Public investments and policies play a significant role in shaping the distribution of resources and opportunities to be healthy, so reducing disparities in health outcomes requires directing more resources to the communities that have faced the greatest barriers to health, training providers to address racism, and increasing the diversity of the health care workforce. Policies shape where people can afford to live and whether those places are served by grocery stores with fresh foods, public transit that reduces car dependence, and public parks and recreation spaces that provide safe places to be active.d All these policies, in addition to closing the Medicaid coverage gap, must be addressed to advance health equity.
a Jamila Taylor et al., “Eliminating Racial Disparities in Maternal and Infant Mortality: A Comprehensive Policy Blueprint,” Center for American Progress, May 2019, https://cdn.americanprogress.org/content/uploads/2019/04/30133000/Maternal-Infant-Mortality-report.pdf?_ga=2.58426478.534167243.1625237322-612833220.1620046882.
b Linda Villarosa, “Why America’s Black Mothers and Babies Are in a Life-or-Death Crisis,” New York Times Magazine, April 11, 2018, https://www.nytimes.com/2018/04/11/magazine/black-mothers-babies-death-maternal-mortality.html.
c National Partnership for Women & Families, “Listening to Black Mothers in California,” September 2018, https://www.nationalpartnership.org/our-work/resources/health-care/maternity/listening-to-black-mothers-in-california.pdf.
d Jennifer Sullivan, “Better State Budget, Policy Decisions Can Improve Health,” Center on Budget and Policy Priorities, February 21, 2019, https://www.cbpp.org/research/state-budget-and-tax/better-state-budget-policy-decisions-can-improve-health.
Maternal Mortality and Morbidity: High and Rising
An estimated 700 to 900 women in the United States die each year from pregnancy-related complications. Black women are about three times more likely to die than white women, and American Indian/Alaska Native women are twice as likely.[1] Most of these deaths are preventable.[2]
For every 100,000 live births in 2018, 17 mothers died — more than twice the maternal mortality rate of most other high-income countries.[3] The rate rose to 20 out of every 100,000 live births in 2019, and 44 maternal deaths for Black women. (See Figure 2.) At least 50,000 people a year experience serious complications of pregnancy, and these complications also disproportionately affect Black women.[4] Latina women do not experience deaths at a higher rate, but are at higher risk for severe maternal morbidity.[5] Notably, a college-educated Black mother is at 60 percent greater risk for maternal death than a white or Latina woman with less than a high school education.[6]

There is now consensus among researchers and health care providers that disproportionately high maternal mortality and morbidity among Black women, regardless of income and education, are due to structural racism in the delivery of health care services along with their lived experiences of racism, which leads to toxic stress and elevated risk of conditions such as hypertension.[7]
Stark Racial Disparities in Risk Factors and Outcomes
Cardiovascular conditions including high blood pressure, heart muscle disease, and blood clots are the leading cause of pregnancy-related deaths. Due in significant part to lasting exposure to adverse experiences including structural racism, Black women are at higher risk for these treatable and preventable conditions.[8] (See box, “People of Color’s Higher Maternal Mortality, Morbidity Rates Rooted in Structural Racism.”) Chronic hypertension is associated not only with pregnancy-related deaths and maternal morbidity but also with significant fetal and neonatal morbidity and mortality.[9] (See box, “Mortality Also Higher for Infants of Black Women.”)
Mortality Also Higher for Infants of Black Women
While infant mortality rates in the United States have fallen over the past decade, they have fallen at a slower rate among infants of Black women than infants of women of other races.a The infant mortality rate among infants of Black women was 10.75 per 1,000 live births, the highest of any racial/ethnic group and nearly twice the national average of 5.67. Maternal complications, preterm birth and low birthweight are among the key causes of infant mortality. Infants born to Black mothers also have higher rates of low birthweight than any other racial/ethnic group for which data are available.b Low-birthweight babies are more likely to experience serious health complications as infants and are at higher risk for harmful health conditions like heart disease and high blood pressure later in life.
In addition to addressing maternal morbidity and mortality, closing the Medicaid coverage gap would be a down payment on better health outcomes for Black infants and children. More than 70 percent of children in low-income families are enrolled in Medicaid.c Improving access to prenatal and postpartum health care will contribute to better health outcomes for children, especially children enrolled in Medicaid.
a U.S. Department of Health and Human Services, “Health, United States: 2019,” https://www.cdc.gov/nchs/data/hus/hus19-508.pdf.
b National Vital Statistics Reports, “Births: Final Data for 2019,” Centers for Disease Control and Prevention, March 23, 2021, https://www.cdc.gov/nchs/data/nvsr/nvsr70/nvsr70-02-508.pdf.
c State Health Facts, “Health Insurance Coverage of Low Income Children 0-18 (under 200% FPL),” 2019, https://www.kff.org/other/state-indicator/health-insurance-coverage-of-low-income-children-0-18-under-200-fpl/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
Racial disparities are significant in the rate of severe maternal morbidity: it was 63 percent higher for women in majority Black and 32 percent higher in majority Latino communities in 2020 than in majority white communities, according to a study of claims for 2.2 million hospital deliveries with a major insurer. The same study found women in majority Black communities have up to twice the prevalence of risk factors such as hypertension or anemia than women in majority white communities. Women in majority Latino communities have prevalence rates up to a third higher for a prior cesarean birth and preexisting diabetes, which are also risk factors for severe maternal morbidity.[10] Having health coverage before and between pregnancies makes it far more likely that these risks get screened for and treated prior to pregnancy, thereby decreasing the risk of poor outcomes.
Medicaid Key to Addressing Maternal Mortality and Morbidity
Medicaid and the Children’s Health Insurance Program (CHIP) pay for more than 40 percent of births in the United States, ranging from a high of 71 percent in New Mexico to a low of 20 percent in Vermont. Medicaid pays for at least 50 percent of births in all states that haven’t expanded Medicaid except for Wisconsin.[11] The share of births that Medicaid finances is higher for Black and Latina women, at 65 percent and 59 percent in 2019, respectively.[12]
Medicaid’s importance in covering pregnant people is especially apparent when looking at how Medicaid coverage of women of reproductive age increases after they become pregnant and decreases afterwards. In 2017, 13.2 percent of women of reproductive age reported being uninsured prior to pregnancy. But the share dropped sharply to 2.6 percent during pregnancy and returned to 10.8 percent after pregnancy. These fluctuations corresponded to increases in Medicaid coverage for this group, which went from 23 percent prior to pregnancy to 35.6 percent during pregnancy and 29.7 percent after.[13]
States must cover pregnant people with incomes up to 133 percent of the poverty line and all but four states cover people with higher incomes, with the 2021 median eligibility level among all states at 200 percent of the poverty line.[14] Pregnancy coverage continues through 60 days postpartum, and the American Rescue Plan Act gives states the option to make postpartum coverage available for 12 months, beginning April 1, 2022.[15] Three states are already providing extended postpartum coverage through demonstrations under Social Security Act section 1115, two states have proposals pending, and 17 have enacted legislation or taken other steps to extend postpartum coverage.[16]
All states should take up the option to extend postpartum coverage, but that doesn’t go far enough. In states that haven’t expanded Medicaid, many people have to wait until they become pregnant to get coverage. States that haven’t expanded generally only cover parents with very low incomes; adults without children generally don’t have any pathway to coverage regardless of their income. The median non-expansion state caps eligibility for parents at about 40 percent of the poverty line, or just $8,800 in annual income for a single parent with two children.[17]
There were just over 800,000 uninsured women of reproductive age in the Medicaid coverage gap in 2019. Most of these women lived in the South, with over 300,000 in Texas alone, and almost two-thirds were people of color (29 percent were Black and 33 percent were Latino).[18] These women could enroll in Medicaid if they become pregnant, but they have no pathway to coverage until they know they are pregnant and apply for and enroll in Medicaid. This leaves them without access to care that could identify and address their health risks before pregnancy and potentially delays the start of prenatal care.[19]
Closing the Coverage Gap Lays Foundation to Improve Outcomes
Extending postpartum coverage, as the American Rescue Plan allows states to do, is critically important to reducing maternal mortality and morbidity. That is because about a third of deaths, most of which are preventable, occur between seven and 365 days following delivery.[20] Other Medicaid proposals, such as covering doulas, expanding coverage for home visiting programs that support pregnant people and new parents, and providing evidence-informed services to pregnant people with behavioral health conditions also would contribute to better outcomes for both parents and babies, as would improvements in housing, transportation, nutrition, and environmental conditions.[21] Doulas in particular have been effective in supporting Black women through pregnancy, childbirth, and the postpartum period.[22]
But fully addressing maternal mortality and morbidity, especially for Black women, requires attention to people’s health before and between pregnancies. Having care in these periods allows for identification and treatment of risk factors such as hypertension and diabetes as well as for preconception health care services such as counseling and prescriptions for folic acid, which reduces birth defects. Women who are uninsured before pregnancy are more likely to have these risk factors that are associated with worse outcomes.[23] Moreover, having Medicaid before and between pregnancies ensures access to family planning services and supplies, which all states must cover. Contraceptive use reduces maternal mortality not just in the United States, but around the world, research shows.[24]
Having coverage before pregnancy also eliminates the gap in coverage that occurs between conception and being found eligible for Medicaid based on pregnancy. Nationwide, just 68 percent of people whose births were financed by Medicaid had prenatal care that began in the first trimester.[25]
Medicaid Expansion Decreased Uninsured Rate for Women of Reproductive Age Prior to Pregnancy
Overall, Medicaid expansion decreased the uninsured rate for women of reproductive age by 13.2 percentage points, one study estimated.[26] The decrease was much greater, 27.4 percentage points, for women without dependent children who weren’t eligible for Medicaid prior to expansion than it was for parents, some of whom qualified before expansion.
Expansion states also had lower uninsurance rates among women both before and after pregnancy, according to a 43-state study of new mothers who had Medicaid-covered prenatal care between 2015 and 2018. In expansion states, 17.3 percent of new mothers were uninsured prior to conception, less than half the uninsured rate for mothers in non-expansion states (38.1 percent). Within two to six months postpartum, just 10 percent of mothers in expansion states became uninsured compared to 36.1 percent in non-expansion states.[27] Medicaid expansion resulted in a 10.1 percentage-point decrease in churn, defined as moving between different insurance plans or between insurance and uninsurance, according to another study of 19 states and New York City covering 2012 to 2017.[28]
Medicaid Expansion Increased Preconception Health Care
Having coverage makes a difference in the care pregnant people receive. Medicaid expansion was associated with a 22 percent increase in preconception health counseling aimed at addressing risks such as smoking, depression, uncontrolled diabetes, and hypertension before conception. Expansion also led to a 10 percent increase in the proportion of women with low incomes who reported daily folic acid intake in the month before conception. While expansion did not lead to significant changes in indicators related to chronic disease or other health behaviors, researchers noted that the study period of five years after expansion took effect may have been too short to observe detectable changes.[29]
An Oregon study found that expansion, two years after its implementation, increased Medicaid enrollment prior to pregnancy and also increased timely and adequate prenatal care.[30] Medicaid expansion has also been shown to be associated with increased utilization of health care, better self-rated health, and decreased avoidance of health care due to costs among women of reproductive age.[31]
Medicaid Expansion Associated With Lower Maternal Mortality and Morbidity
A recent study of maternal mortality from 2006 to 2017 found that while the overall maternal mortality ratio (deaths per 100,000 live births) rose over the period, it was lower in expansion versus non-expansion states. The difference was greatest among Black mothers and was also significant for Hispanic mothers.[32] And in New York, expansion was associated with a statistically significant reduction in severe maternal morbidity among women with low incomes.[33] An editorial accompanying the study notes the importance of preconception care in optimizing women’s health, managing chronic disease, and addressing risk factors for women and their babies.[34]
These studies confirm that coverage will be key to reducing maternal mortality and morbidity for women of color. That coverage must be comprehensive and offer evidence-informed services that are free of discrimination. And it must identify and reduce risks associated with poor pregnancy outcomes for women of color, including those due to toxic stress, poverty, and racism.
| APPENDIX TABLE 1 | ||||||
|---|---|---|---|---|---|---|
| Uninsured Women of Reproductive Age in the Coverage Gap, by Race/Ethnicity (Southern States) | ||||||
| State | Total | Black | Latina | White | Other | |
| Alabama | 51,000 | 22,000 | * | 28,000 | * | |
| Florida | 130,000 | 40,000 | 40,000 | 44,000 | 7,000 | |
| Georgia | 100,000 | 50,000 | 12,000 | 36,000 | * | |
| Mississippi | 43,000 | 25,000 | * | 15,000 | * | |
| North Carolina | 73,000 | 24,000 | 8,000 | 36,000 | * | |
| South Carolina | 34,000 | 14,000 | * | 16,000 | * | |
| Tennessee | 31,000 | 8,000 | * | 20,000 | * | |
| Texas | 324,000 | 48,000 | 193,000 | 72,000 | 11,000 | |
End Notes
[1] Samantha Artiga et al., “Racial Disparities in Maternal and Infant Health: An Overview,” Kaiser Family Foundation, November 10, 2020, https://www.kff.org/report-section/racial-disparities-in-maternal-and-infant-health-an-overview-issue-brief/.
[2] Emily E. Petersen et al., “Vital Signs: Pregnancy-Related Deaths, United States, 2011-2015, and Strategies for Prevention, 13 States, 2013-2017,” Morbidity and Mortality Weekly Report, Centers for Disease Control and Prevention, May 10, 2019, https://www.cdc.gov/mmwr/volumes/68/wr/mm6818e1.htm?s_cid=mm6818e1_w.
[3] Roosa Tikkanen et al.,¸“Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries,” Commonwealth Fund, November 1, 2020, https://www.commonwealthfund.org/publications/issue-briefs/2020/nov/maternal-mortality-maternity-care-us-compared-10-countries.
[4] Gianna Melillo, “Racial Disparities Persist in Maternal Morbidity, Mortality and Infant Health,” AJMC, June 13, 2020, https://www.ajmc.com/view/racial-disparities-persist-in-maternal-morbidity-mortality-and-infant-health.
[5] Artiga et al., op cit.
[6] Eugene Declercq and Laurie Zephyrin, “Maternal Mortality in the United States: A Primer,” Commonwealth Fund, December 16, 2020, https://www.commonwealthfund.org/publications/issue-brief-report/2020/dec/maternal-mortality-united-states-primer.
[7] Linda Villarosa, “Why America’s Black Mothers and Babies Are in a Life-or-Death Crisis,” New York Times Magazine, April 11, 2018, https://www.nytimes.com/2018/04/11/magazine/black-mothers-babies-death-maternal-mortality.html.
[8] Declercq and Zephyrin, op. cit.
[9] “Putting America’s Health First,” FY 2021 President’s Budget for HHS, https://www.hhs.gov/sites/default/files/fy-2021-budget-in-brief.pdf.
[10] Blue Cross Blue Shield, “Racial Disparities in Maternal Health,” May 20, 2021, https://www.bcbs.com/sites/default/files/file-attachments/health-of-america-report/BCBSA-HOA-Maternal_Health_Dispairities.pdf.
[11] Kaiser Family Foundation State Health Facts, “Births Financed by Medicaid,” https://www.kff.org/medicaid/state-indicator/births-financed-by-medicaid/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Percent%20of%20Births%20Financed%20by%20Medicaid%22,%22sort%22:%22desc%22%7D.
[12] Joyce A. Martin, Brady E. Hamilton, and Michelle J.K. Osterman, “Births in the United States, 2019,” Centers for Disease Control and Prevention, NCHS Data Brief No. 387, October 2020, https://www.cdc.gov/nchs/data/databriefs/db387-H.pdf.
[13] Centers for Medicare & Medicaid Services, “Medicaid and CHIP Beneficiary Profile: Maternal and Infant Health,” December 2020, https://www.medicaid.gov/medicaid/quality-of-care/downloads/mih-beneficiary-profile.pdf.
[14] Kaiser Family Foundation State Health Facts, “Medicaid and CHIP Income Eligibility Limits for Pregnant Women as a Percent of the Federal Poverty Level,” as of January 1, 2021, https://www.kff.org/health-reform/state-indicator/medicaid-and-chip-income-eligibility-limits-for-pregnant-women-as-a-percent-of-the-federal-poverty-level/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. States may also cover pregnant people in CHIP through a state option or section 1115 demonstration program, but none of the non-expansion states have done so.
[15] A maintenance of effort requirement associated with the 6.2 percentage-point increase in federal matching funds prohibits states from terminating coverage during the coronavirus public health emergency, which is expected to last throughout 2021, so pregnant people can currently remain eligible for longer than 60 days postpartum.
[16] Seven non-expansion states — Florida, Georgia, North Carolina, South Carolina, Tennessee, Texas, and Wisconsin — are among the states that have extended or plan to extend postpartum coverage. Kaiser Family Foundation, “Medicaid Postpartum Coverage Extension Tracker,” July 15, 2021, https://www.kff.org/medicaid/issue-brief/medicaid-postpartum-coverage-extension-tracker/.
[17] The exception is Wisconsin, which extends Medicaid eligibility to adults with incomes up to 100 percent of the poverty line.
[18] Gideon Lukens and Breanna Sharer, “Closing Medicaid Coverage Gap Would Help Diverse Group and Narrow Racial Disparities,” Center on Budget and Policy Priorities, revised June 14, 2021, https://www.cbpp.org/research/health/closing-medicaid-coverage-gap-would-help-diverse-group-and-narrow-racial; data on race/ethnicity of women of reproductive age from CBPP analysis of the 2019 American Community Survey. See Appendix II of Lukens and Sharer for details on methodology.
[19] Thirty states, including seven non-expansion states (Florida, Georgia, Kansas, North Carolina, Tennessee, Texas, and Wisconsin) provide presumptive eligibility for pregnant people, which allows providers and other approved entities to make a preliminary determination of Medicaid eligibility with a full determination afterward. But even in those states, eligibility and provider payments don’t begin until pregnancy is confirmed. Kaiser Family Foundation State Health Facts, “Presumptive Eligibility in Medicaid and CHIP,” as of January 1, 2020, https://www.kff.org/health-reform/state-indicator/presumptive-eligibility-in-medicaid-chip/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. South Carolina did not report whether it provides presumptive eligibility.
[20] Petersen et al., op cit.; Medicaid and CHIP Payment and Access Commission, “Advancing Maternal and Infant Health by Extending the Postpartum Coverage Period,” Report to Congress on Medicaid and CHIP, March 2021, https://www.macpac.gov/wp-content/uploads/2021/03/Chapter-2-Advancing-Maternal-and-Infant-Health-by-Extending-the-Postpartum-Coverage-Period.pdf.
[21] See, for example, the “Black Maternal Health Momnibus,” a package of 12 bills introduced by the Black Maternal Health Caucus of the House of Representatives, https://blackmaternalhealthcaucus-underwood.house.gov/Momnibus, and Jamila Taylor et al., “Eliminating Racial Disparities in Maternal and Infant Mortality: A Comprehensive Policy Blueprint,” Center for American Progress, May 2019, https://cdn.americanprogress.org/content/uploads/2019/04/30133000/Maternal-Infant-Mortality-report.pdf?_ga=2.58426478.534167243.1625237322-612833220.1620046882.
[22] Villarosa, op. cit. Four states (Indiana, Minnesota, New Jersey, and Oregon) cover doulas in their Medicaid programs, and New York has a pilot program. Ashley Nguyen, “Behind the growing movement to include doulas under Medicaid,” Washington Post, March 1, 2021, https://www.washingtonpost.com/graphics/2021/the-lily/covering-doulas-medicaid/.
[23] Cheryl Robbins et al., “Disparities in Preconception Health Indicators — Behavioral Risk Factor Surveillance System, 2013-2015, and Pregnancy Risk Assessment Monitoring System, 2013-2014,” Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, January 19, 2018, https://www.cdc.gov/mmwr/volumes/67/ss/ss6701a1.htm.
[24] Saifuddin Ahmed et al., “Maternal deaths averted by contraceptive use: an analysis of 172 countries,” The Lancet, July 14, 2012, https://www.thelancet.com/action/showPdf?pii=S0140-6736%2812%2960478-4.
[25] Medicaid and CHIP Payment and Access Commission, “Medicaid’s Role in Maternal Health,” Report to Congress on Medicaid and CHIP, June 2020, https://www.macpac.gov/wp-content/uploads/2020/06/Chapter-5-Medicaid%E2%80%99s-Role-in-Maternal-Health.pdf.
[26] Emily M. Johnston et al., “Impacts of the Affordable Care Act’s Medicaid Expansion on Women of Reproductive Age: Differences by Parental Status and State Policies,” Women’s Health Issues, March 1, 2018, https://www.whijournal.com/article/S1049-3867(17)30242-6/fulltext.
[27] Emily M. Johnston et al., “Post-ACA, More Than One-Third Of Women With Prenatal Medicaid Remained Uninsured Before Or After Pregnancy,” Health Affairs, April 2021, https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2020.01678.
[28] Jamie R. Daw et al., “Medicaid Expansion Improved Perinatal Insurance Continuity For Low-Income Women,” Health Affairs, September 2020, https://www.healthaffairs.org/doi/10.1377/hlthaff.2019.01835.
[29] Rebecca Myerson et al., “Medicaid Expansion Increased Preconception Health Counseling, Folic Acid Intake, And Postpartum Contraception,” Health Affairs, November 2020, https://www.healthaffairs.org/doi/10.1377/hlthaff.2020.00106.
[30] S. Marie Harvey, et al., “Impact of Medicaid expansion in Oregon on access to prenatal care,” Preventive Medicine, February 2021, https://www.sciencedirect.com/science/article/abs/pii/S0091743520303911?via%3Dihub.
[31] Claire E. Margerison et al., “Impacts of Medicaid Expansion on Health Among Women of Reproductive Age,” American Journal of Preventive Medicine, January 1, 2020, https://www.ajpmonline.org/article/S0749-3797(19)30373-3/fulltext.
[32] Erica L. Eliason, “Adoption of Medicaid Expansion Is Associated with Lower Maternal Mortality,” Women’s Health Issues, February 25, 2020, https://www.whijournal.com/article/S1049-3867(20)30005-0/fulltext.
[33] Jean Guglielminotti, Ruth Landau, and Guohua Li, “The 2014 New York State Medicaid Expansion and Severe Maternal Morbidity During Delivery Hospitalizations,” Anesthesia and Analgesia, August 2021, https://journals.lww.com/anesthesia-analgesia/Abstract/2021/08000/The_2014_New_York_State_Medicaid_Expansion_and.9.aspx#related.
[34] Lindsay K. Admon and Jamie R. Daw, “Evidence From New York: Perinatal Insurance Expansions as a Lever to Address Maternal Morbidity,” August 2021, Anesthesia and Analgesia, https://journals.lww.com/anesthesia-analgesia/Citation/2021/08000/Evidence_From_New_York__Perinatal_Insurance.8.aspx.
More from the Authors
