Medicaid Expansion Is Producing Large Gains in Health Coverage and Saving States Money
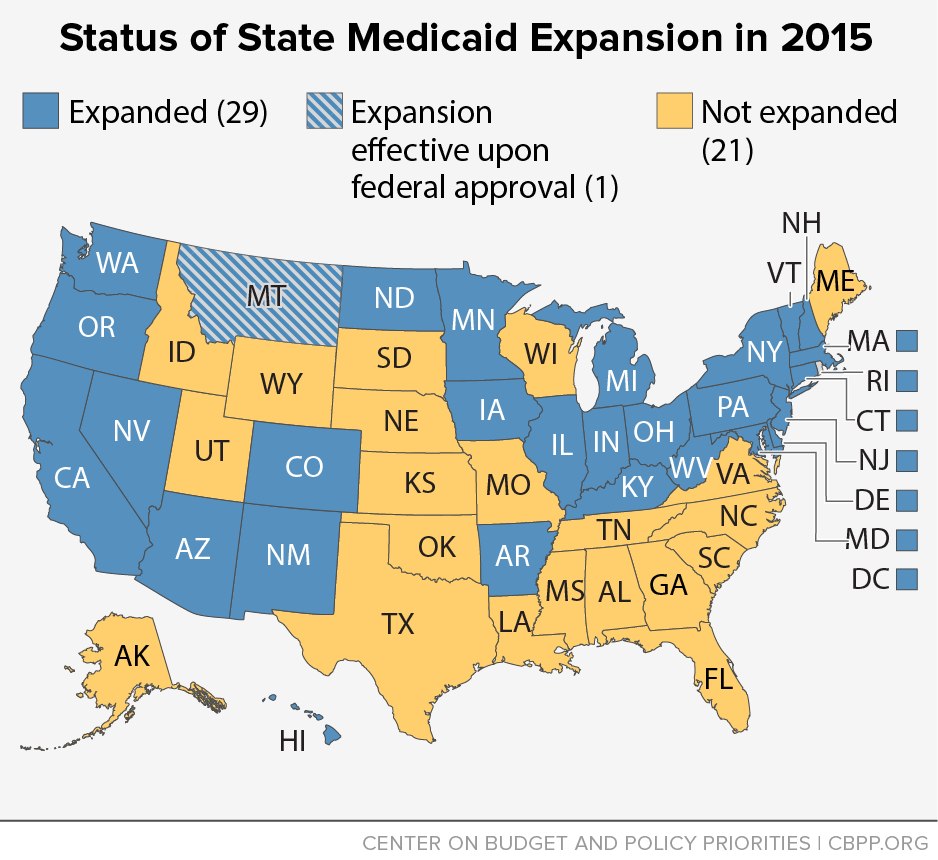
In the short time since states have been able to expand Medicaid to low-income adults under health reform, a clear divide has emerged between states that have expanded Medicaid and those that have not. (See Figure 1.) Since the major coverage provisions of the Affordable Care Act (ACA) took effect in 2014, insurance coverage rates have improved across the country, but the gains are far greater in the states that have expanded Medicaid.[1] As a result, hospitals in expansion states are treating fewer uninsured patients, and the amount of uncompensated care they are providing is declining steeply. Moreover, contrary to critics’ claims that Medicaid expansion is financially unsustainable for states, there is increasing evidence that expansion has saved states money, and these savings are expected to grow over time.
The Medicaid expansion has had an especially dramatic impact in Arkansas and Kentucky, which both had high uninsurance rates and limited Medicaid eligibility for non-elderly adults before health reform. Both states’ uninsurance rates have fallen by half in just over a year, and the expansion is expected to save each state more than $100 million by the time their current state fiscal years end on June 30.
Meanwhile, the states that have not expanded Medicaid are falling further behind. In the non-expansion states, large numbers of low-income people remain uninsured and without access to affordable health coverage. These individuals are caught in a “coverage gap” because their incomes are too high for Medicaid but too low for subsidies to purchase coverage in the marketplace. Hospitals in these states continue to provide large amounts of uncompensated care, and the states are missing the opportunity to leverage billions of dollars in new federal funding through the Medicaid expansion.
States Expanding Medicaid Have Made Greater Health Coverage Gains
The uninsurance rate for adults nationwide dropped from 17.1 percent at the end of 2013, just before the ACA’s major coverage provisions took effect, to 11.9 percent during the first quarter of this year, according to a Gallup and Healthways survey.[2] These results are consistent with other independent and federal government surveys of insurance coverage.[3]
States that expanded Medicaid experienced the greatest gains in health coverage. In just one year, Arkansas and Kentucky cut their uninsurance ratesin half, from 22.5 to 11.4 percent and from 20.4 to 9.8 percent, respectively. Other Medicaid expansion states with large drops in their uninsurance rates include Oregon (19.4 to 11.7 percent), Washington (16.8 to 10.1 percent), and West Virginia (17.6 to 10.9 percent). Nine of the ten states with the largest drops in uninsurance rates are Medicaid expansion states.[4]
Expanding Medicaid Has Saved States Money
Besides producing large gains in coverage, Medicaid expansion is a good fiscal deal for states.
- The federal government is covering the entirecost of the expansion through 2016, and no less than 90 percent of the cost in subsequent years.
- As more uninsured individuals obtain coverage, demand for health care services that serve low-income uninsured residents and are entirely state-funded declines. These programs include treatment for people with mental illness and substance abuse disorders, funding for hospitals to offset their uncompensated care costs, and care for prisoners who have to be hospitalized outside of correctional facilities.
- Expanding Medicaid also allows states to move some people who received services through targeted Medicaid programs at the state’s regular matching rate into the new Medicaid expansion eligibility group with its more generous matching rate. These targeted programs include care for certain women with breast or cervical cancer, family planning services, and medically needy spend-down programs, which allow individuals with high medical expenses to receive coverage by “spending down” their income on medical costs to reach Medicaid eligibility levels.
- Because more people have health coverage, states are collecting more revenue from their existing taxes on health providers and health plans, such as the managed care plans that serve Medicaid beneficiaries in many states.[5]
Among the states that have documented significant budget savings from the Medicaid expansion are:
-
Arkansas: Medicaid expansion saved Arkansas $30.8 million in fiscal year 2014, and the state expects to save an additional $88.8 million in fiscal year 2015, according to state officials interviewed by the State Health Reform Assistance Network. (The $88.8 million in 2015 savings includes $17.2 million in uncompensated care savings and $7.1 million in savings in behavioral health care spending — i.e., spending on mental health care and treatment for substance abuse.)
The cumulative savings of nearly $120 million by the end of fiscal year 2015 include $72.9 million in savings within the Arkansas Medicaid program from moving people who previously received care under specialized Medicaid categories for disabled adults, women with breast or cervical cancer, and others into the expansion’s new eligibility group, for which the federal government pays the full cost. In addition to this nearly $120 million in reduced state expenditures, the state expects to collect $34.4 million in new revenue over 2014 and 2015 from taxes on providers and health plans, producing a total gain for the state budget of over $150 million in 18 months.[6]
- Kentucky: Medicaid expansion saved Kentucky $25.8 million in fiscal year 2014, and is expected to lead to another $83.1 million in savings in fiscal year 2015, according to an analysis prepared for the state by Deloitte Consulting. Among these two-year savings are $30 million from a drop in state spending on behavioral health programs, $16.4 million from spending less on inpatient hospital costs for prisoners, and $16.4 million from moving people who previously received Medicaid coverage through a medically needy spend-down program into the expansion’s new eligibility group.[7]
- Michigan: Medicaid expansion saved the state $180 million in fiscal year 2014 and is projected to save Michigan $190 million in the state’s current fiscal year, which runs through September 30, according to an analysis prepared by the State Health Reform Assistance Network. The savings are primarily from a drop in demand for state-funded community mental health programs. In addition, the state projects two-year savings of $19.2 million in its corrections system, as the federal government now covers the costs of prisoners hospitalized outside the corrections system, as a result of the Medicaid expansion.[8]
- New Jersey: As a result of the Medicaid expansion, Governor Chris Christie’s fiscal year 2016 budget proposal spends $148 million less on charity care and $417 million less on beneficiaries previously covered at the state’s regular matching rate of 50 percent but now covered with 100 percent federal funds, according to state budget documents.[9] The state expects the latter category to result in nearly $3 billion in savings to the state through 2020.[10]
- New Mexico: New Mexico will save $60 million from 2014 to 2016 by transitioning low-income adults who were receiving Medicaid coverage through a waiver prior to health reform into the expansion eligibility group, according to state budget documents. The state expects to save an additional $15.3 million in the current fiscal year because of lower demand for state-funded behavioral health services.[11] The state also collected $30 million in new revenue in 2014 and expects to collect another $30 million this year from its premium taxes that are levied on the managed care plans that serve the new eligibility population.[12]
- Washington: Medicaid expansion saved Washington $105.5 million in fiscal year 2014, and the state expects to save an additional $286.6 million in fiscal year 2015, according to interviews with state officials and an analysis of state budget documents conducted by the Kaiser Family Foundation. Among the savings are $64.6 million in reduced behavioral health spending and $147.9 million from transferring adults awaiting a disability determination for Supplemental Security Income coverage from a state-funded program to Medicaid. The state also expects the Medicaid expansion to contribute to a $33.9 million increase in premium tax revenue in fiscal year 2015.[13]
- West Virginia: The state saved $3.8 million in 2014 as women in the new eligibility group who became pregnant remained in the new eligibility group throughout their pregnancies, rather than moving into the pregnant woman eligibility category, for which the federal government pays the state’s regular matching rate.[14]
Expanding Medicaid Means Hospitals Treat Fewer Uninsured Patients and Provide Less Uncompensated Care
Almost immediately after the ACA’s major coverage provisions took effect in 2014, hospitals in states that expanded Medicaid reported higher-than-expected revenues along with a shift to providing more care to patients with Medicaid coverage and less to uninsured patients.[15] In contrast, hospitals in states that did not expand generally experienced a small-to-negligible drop in their volume of uninsured patients.[16]
The experience of various hospital systems that operate hospitals in both expansion and non-expansion states provides strong evidence of the Medicaid expansion’s impact on hospitals. Between the second quarter of 2013 and the second quarter of 2014, Community Health Systems experienced a 72 percent drop in uninsured admissions at its hospitals in 12 states that expanded Medicaid and no change at its hospitals in 17 states that did not expand. Other hospital systems had similar results: LifePoint experienced a 67 percent reduction in uninsured admissions at its hospitals in Medicaid expansion states, compared with a 14 percent drop in non-expansion states; Tenet’s uninsured admissions fell 54 percent at its hospitals in expansion states compared with an 8 percent drop in non-expansion states; and the Hospital Corporation of America’s uninsured admissions dropped 48 percent at hospitals in expansion states compared with a 2 percent drop in non-expansion states.[17]
Hospital associations in Medicaid expansion states also noted immediate positive impacts from the Medicaid expansion. The Arkansas Hospital Association reported that inpatient admissions of uninsured patients in Arkansas hospitals fell by 46.5 percent between the first six months of 2013 and the first six months of 2014, and emergency room visits by uninsured patients fell 35.5 percent.[18] The Arizona Hospital Association reported a 31 percent drop in the amount of uncompensated care provided by hospitals in the state between April 2013 and April 2014.[19]
Conclusion
Health reform’s Medicaid expansion has proven successful for the states that have taken the option, reducing both their uninsured populations and their health care-related costs and producing budgetary savings. Meanwhile, policymakers in non-expansion states — many of which have high uninsurance rates, limited Medicaid eligibility for parents, and no eligibility for poor adults without children — have forgone significant savings and have placed the burden from their decision not to expand on their poorest residents. In the non-expansion states, 3.7 million uninsured adults remain in a “coverage gap,” with incomes too high for Medicaid but too low for subsidies to buy coverage in the marketplace.[20] The evidence from expansion states shows that these adults — and the states where they live — would benefit from the Medicaid expansion.
End Notes
[1] Twenty-eight states and the District of Columbia have implemented the Medicaid expansion. This does not include Montana, where the legislature approved a Medicaid expansion on April 18, contingent upon the state gaining federal approval for a waiver.
[2] Jenna Levy, “In U.S., Uninsured Rate Dips to 11.9% in First Quarter,” Gallup, April 13, 2015, http://www.gallup.com/poll/182348/uninsured-rate-dips-first-quarter.aspx.
[3] Like the Gallup and Healthways survey, one government survey and three additional independent surveys all show a significant reduction in the share of non-elderly adults without health insurance coverage since the major coverage provisions of the ACA took effect in 2014. Results vary slightly due both to differences in survey methodology and the period of time captured. These surveys — from the Centers for Disease Control and Prevention, the Urban Institute, RAND, and the Commonwealth Fund — all estimate that the uninsured rate among non-elderly adults has been reduced by between one-fifth and nearly one-half since late 2013. For more information on these survey results, see Matt Broaddus and Edwin Park, “Understanding the Census Bureau’s Upcoming Health Insurance Coverage Estimates,” Center on Budget and Policy Priorities, September 11, 2014, https://www.cbpp.org/research/understanding-the-census-bureaus-upcoming-health-insurance-coverage-estimates?fa=view&id=4199#privateSurveysShow.
[4] Montana, which had the ninth-largest drop in its uninsured rate, was the one non-expansion state in the top ten. Montana’s legislature recently approved expansion once the state secures a waiver from the federal government to do so. Dan Witters, “Arkansas, Kentucky See Most Improvement in Uninsured Rates,” Gallup, February 24, 2015, http://www.gallup.com/poll/181664/arkansas-kentucky-improvement-uninsured-rates.aspx.
[5] For more information on the Medicaid expansion’s potential impacts on state budgets, see January Angeles, “How Health Reform’s Medicaid Expansion Will Impact State Budgets,” Center on Budget and Policy Priorities, revised July 25, 2012, https://www.cbpp.org/cms/index.cfm?fa=view&id=3801.
[6] Deborah Bachrach, Patricia Boozang, and Dori Glanz, “States Expanding Medicaid See Significant Budget Savings and Revenue Gains,” State Health Reform Assistance Network, April 2015, http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2015/rwjf419097. Arkansas’ figures are based on interviews with state officials.
[7] See Bachrach, op cit. Kentucky’s figures are based on a February 2015 analysis prepared for the state of Kentucky by Deloitte Consulting, http://governor.ky.gov/healthierky/Documents/medicaid/Kentucky_Medicaid_Expansion_One-Year_Study_FINAL.pdf.
[8] Bachrach, op cit.
[9] Andrew Kitchenman, “Christie’s Budget Cuts $148M from Hospital Charity Care,” New Jersey Public Radio, February 25, 2015, http://www.wnyc.org/story/christies-budget-cuts-148m-hospital-charity-care/.
[10] Based on documents from the state’s Department of Human Services’ Division of Management and Budget.
[11] New Mexico Legislative Finance Committee, 2014 Post-Session Review, April 2, 2014, http://www.nmlegis.gov/lcs/lfc/lfcdocs/April%202014.pdf.
[12] Bachrach, op cit.
[13] Stan Dorn, Norton Francis, Laura Snyder, and Robin Rudowitz, “The Effects of the Medicaid Expansion on State Budgets: An Early Look in Select States,” Kaiser Family Foundation, March 11, 2015, http://files.kff.org/attachment/issue-brief-the-effects-of-the-medicaid-expansion-on-state-budgets-an-early-look-in-select-states.
[14] Bachrach, op cit.
[15] For-profit health systems like Community Health Systems, HCA, and LifePoint all reported greater-than-expected revenues in the first half of 2014, especially from their hospitals in Medicaid expansion states. Pricewaterhouse Coopers, “The health system haves and have nots of ACA expansion,” September 2014, http://www.pwc.com/us/en/health-industries/health-research-institute/assets/pwc-hri-medicaid-report-final.pdf.
[16] Thomas DeLeire, Karen Joynt, and Ruth McDonald, “Impact of Insurance Expansion on Hospital Uncompensated Care Costs in 2014,” US Department of Health and Human Services, September 11, 2014, http://aspe.hhs.gov/health/reports/2014/uncompensatedcare/ib_uncompensatedcare.pdf.
[17] DeLeire, Joynt, and McDonald, op cit.
[18] Paul Cunningham, editor, “Survey Reveals Private Option Impact on Hospitals,” Arkansas Hospital Association, November 3, 2014, http://www.arkhospitals.org/archive/notebookpdf/Notebook_11-03-14.pdf.
[19] Jim Haynes, “April 2014 Hospital Financial Results,” Arizona Hospital and Healthcare Association, June 13, 2014.
[20] Rachel Garfield, Anthony Damico, Jessica Stephens, and Saman Rouhani, “The Coverage Gap: Uninsured Poor Adults in States that Do Not Expand Medicaid — An Update,” Kaiser Family Foundation, November 2014, http://files.kff.org/attachment/the-coverage-gap-uninsured-poor-adults-in-states-that-do-not-expand-medicaid-issue-brief.
More from the Authors
