
WILL THE NEW TENNCARE
CUTBACKS HELP
by Leighton Ku
| PDF of analysis |
|
| If you cannot access the files through the links, right-click on the underlined text, click "Save Link As," download to your directory, and open the document in Adobe Acrobat Reader. |
The state of
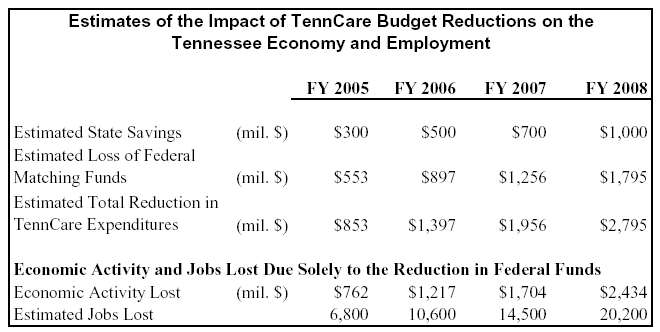
Gov. Bredesen’s office has stated that the new
TennCare policies will substantially reduce state expenditures in the coming
years. The cutbacks are estimated to lower state expenditures by $300 million
in FY 2005, an amount which rises to $1.0 billion by FY 2008.[2]
While these policies would lower state budget expenditures, they also would
adversely affect
The combined loss of state and federal dollars means that hospitals, physicians, pharmacists, nursing homes and other health care providers throughout the state would have lower TennCare revenues in the coming years. In turn, this means that these providers would employ fewer staff, purchase fewer medical supplies, and so on. In many parts of the state, particularly rural areas, the reduction in TennCare revenues would make it harder for clinics or other health care facilities to keep their doors open or to offer the breadth of services they now provide. For many health care providers, TennCare is a major revenue source, and a reduction in TennCare funds can have substantial repercussions for their operations.
Additional ripple effects would be felt in other
parts of
This analysis uses information about
Given those caveats, our analyses indicate the new TennCare cutbacks would result in:
- A loss of federal matching funds that rises from $550 million in FY 2005 to $1.8 billion in FY 2008.
- A total reduction in TennCare expenditures of $850 million in FY 2005 and $2.8 billion in FY 2008.
-
A substantial reduction in total economic activity in
-
Thousands of jobs lost in
These analyses should be considered conservative. They do not account for reductions in the state’s share of TennCare spending that could affect economic activity, or for further budget reductions that might occur due to changes in the definition of medical necessity in determining whether TennCare will cover certain health care services provided to beneficiaries.
Our estimates also do not account for the
possibility that some patients’ medical conditions will worsen because they do
not receive the most appropriate medical care or are unable to get needed
prescription drugs in TennCare and therefore could require more intensive or
expensive medical treatment at a later time.[3]
A recent study found, for example, that patients who limited their use of
medications because they could not afford them were more likely to have heart
attacks or strokes, and another study found that increased copayments for
prescription drugs led poor patients to use fewer medications but resulted in
increased hospital and emergency room use.
[4] If we accounted for these factors, the estimated harm
to
Finally, our estimates do not account for the
potential harm or cost to other public services in
Technical Notes
For FFY 2005, the Medicaid matching rate for
The
economic multiplier analyses were derived from analyses for
End Notes:
[1]
William Welch and Julie Appleby, “States Watching Tennessee’s Health Care
Plan for the Poor,” USA Today,
[2] These are rough estimates presented by the Governor’s office. They do not include savings attributable to changes in the definition of medical necessity. If additional savings due to the definition change were included, then all the estimates in this paper would be even larger.
[3] See, for example, S. Soumerai, "Benefits and Risks of Increasing Restrictions on Access to High Cost Drugs in Medicaid", Health Affairs, 23: 135-146 (Jan./Feb. 2004).
[4] M. Heisler, et al., “The Health Effects of Restricting Prescription Medication Use Because of Cost”, Medical Care, 42(7):626-34, July 2004 and Robyn Tamblyn, et al., “Adverse Events Associated with Prescription Drug Cost-Sharing among Poor and Elderly Persons,” Journal of the American Medical Association, 285(4): 421-429, January 2001.
[5]
Christopher Conover and Hester Davies, The
Role of TennCare in Health Policy for Low-income People in
[6]
Families