Michigan’s Waiver Proposal Would Undermine Its Successful Medicaid Expansion
Michigan’s Medicaid expansion has been extremely successful, extending coverage and access to care to over 1 million low-income adults in Michigan since April 2014 and improving their physical and financial health. The state’s Medicaid expansion — called Healthy Michigan and implemented under the Affordable Care Act (ACA) — currently provides coverage to over 668,000 low-income Michiganders while also providing economic benefits to the state and reducing uncompensated care for hospitals and other safety net providers.[1] But Michigan is putting this well-documented success in jeopardy with its proposal to both impose higher premiums on Medicaid expansion beneficiaries and to take away their coverage if they don’t meet work requirements. Michigan is putting this well-documented success in jeopardy.
Research shows that Michigan’s expansion has:
- Cut Michigan’s uninsured rate in half since expansion began in April 2014.
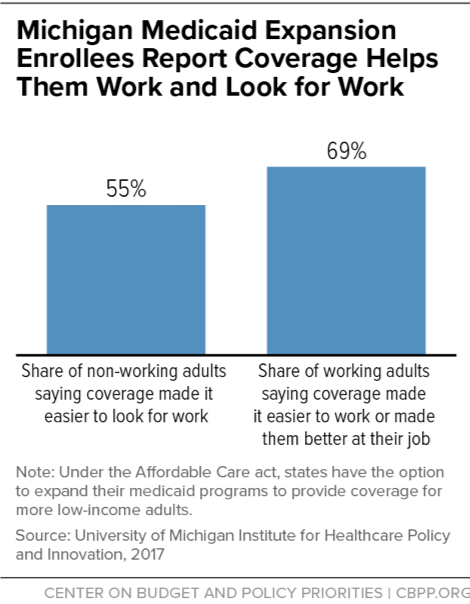
- Made working and searching for work easier. In beneficiary surveys, half of non-working adults reported that having Medicaid made it easier to look for work, and nearly 70 percent of those already working said Medicaid made it easier to work or made them better at their job.
- Improved access to care, as well as detection of serious health conditions and management of chronic health conditions, particularly among beneficiaries who were previously uninsured.
- Improved beneficiaries’ physical health, consistent with nationwide data.
- Improved financial health. After enrolling, Healthy Michigan enrollees had less medical debt, less debt being sent to collectors, and less debt that is past due.
- Provided economic benefits for state and hospital budgets. Medicaid expansion has contributed to improvements in Michigan’s economy by creating jobs, bringing in more tax revenue, and cutting in half the amount of uncompensated care for safety net providers.
Michigan is proposing to take Medicaid away from expansion beneficiaries for not meeting work requirements, and to impose higher premiums on them, through an amendment to its current 1115 Medicaid demonstration, or “waiver.” The proposal will likely lead to significant coverage losses and add new costs to the state’s budget. The Michigan House Fiscal Agency estimates that up to 54,000 Michiganders would lose Medicaid coverage through implementation of the state’s proposal to take Medicaid away from people who don’t meet the work requirement.[2] And recent evidence from Arkansas suggests coverage losses could be even greater, given the thousands who have already lost coverage in that state as a result of similar requirements, and the difficulty in reporting compliance with them.[3]
Section 1115 of the Social Security Act allows the Secretary of Health and Human Services (HHS) to approve demonstration projects that promote Medicaid’s objectives. A “central objective” of Medicaid is providing affordable coverage to people who would otherwise be uninsured, a federal court recently noted in vacating the approval of a Kentucky waiver that included a work requirement and new premiums. Michigan’s waiver, which would lead to significant coverage losses and undermine the gains the state has made in the health and financial well-being of low-income Michiganders, likewise fails to promote Medicaid’s objectives.
Michigan’s Successful Medicaid Expansion
Healthy Michigan began in April 2014 under the authority of a section 1115 waiver, enabling over 1 million Michiganders with incomes below 138 percent of the poverty line who were previously uninsured or underinsured to gain coverage.[4] Like Medicaid expansion nationwide, Healthy Michigan has led to significant progress in cutting Michigan’s uninsured rate, improving access to care and the physical and financial health of Medicaid beneficiaries, and generating revenue and other economic benefits by strengthening the state’s budget and hospital budgets:[5]
- Uninsured rate cut in half. Michigan’s uninsured rate has decreased by 50 percent overall and by at least 40 percent in all but one of the state’s counties since the state implemented Healthy Michigan in 2014.[6] Wayne County, which includes Detroit, has seen a 55 percent drop, while rural Alpena and Gogebic counties have seen drops of 56 and 52 percent, respectively. (See Figure 1.)
- Makes work and searching for a job easier. In a survey of beneficiaries, over half of non-working adults reported that Medicaid makes it easier to look for work, while nearly 70 percent of working adults said Medicaid made it easier to work or made them better at their jobs.[7] (See Figure 2.)
One study of Michigan’s Medicaid expansion showed that more than half of working expansion beneficiaries had a serious physical health condition such as heart disease, asthma, or diabetes, and 25 percent had a mental health condition, often depression.[8] When conditions like diabetes, heart disease, or depression are treated and controlled, individuals with these conditions may be able to hold a steady job. For example, a long-term randomized trial found that providing older adults with regular care for heart disease increased their earnings, likely by reducing their time out of work due to illness.[9] In contrast, if chronic conditions are untreated, work may become impossible. Work requirements can create a vicious cycle in which health setbacks lead to job loss, which in turn leads to loss of access to treatment, making it difficult or impossible to manage health and regain employment.
- Improved access to care. Primary care providers surveyed by Healthy Michigan evaluators, including physicians and nurse practitioners, reported that Medicaid expansion has improved access to care, detection of serious health conditions, and management of chronic health conditions, particularly among beneficiaries who were previously uninsured.[10] The increase in the number of Medicaid beneficiaries did not result in less access to care. The share of health clinics accepting new Medicaid patients increased slightly following Medicaid expansion; and increased appointment availability measured four months following the implementation of expansion remained one year after expansion, one study showed.[11]
- Improved physical health. Nearly 48 percent of enrollees surveyed reported improvement in their physical health since enrolling in the program.[12] Researchers comparing Michigan and Virginia, which hadn’t expanded Medicaid, found that Michigan patients had a lower risk of morbidity and mortality, and that hospitals had fewer uninsured cardiac surgery patients.[13]
- Improved financial health. After enrolling in Healthy Michigan, beneficiaries had less debt sent to collectors, less past-due debt, and were less likely to spend over their credit card limits, according to a recent study of Healthy Michigan administrative data matched to consumer credit reports. The study also found a significant reduction in the number of public records related to financial challenges, such as evictions, bankruptcies, and wage garnishments.[14] This is consistent with findings from the beneficiary survey. The survey also shows that, 86 percent of beneficiaries who had problems paying their medical bills in the 12 months prior to enrolling in Healthy Michigan reported that “problems paying their medical bills got better” after enrollment.[15]
- Economic benefits for state and hospital budgets. Medicaid expansion has helped improve Michigan’s economy, the state’s budget, and the budgets of hospitals across the state. Michigan’s Medicaid expansion is associated with the creation of 30,000 jobs, and increased economic activity resulting from expansion is estimated to bring the state between $145 million and $153 million in additional state tax revenue each year. Michigan has spent $235 million less on mental health and correctional health services for beneficiaries who were previously ineligible for Medicaid, according to the Michigan House Fiscal Agency.[16] The state is also bringing in more tax revenue from increased personal income that helps offset the cost of the state’s share of expansion. Revenue from these sources is estimated to offset the state’s cost of Medicaid expansion through 2021 and very likely to offset the state’s cost in subsequent years.[17]
Hospital budgets have also benefited through lower uncompensated care costs, two recent studies show. Uncompensated care for the average Michigan hospital fell from $8.1 million in 2013 to $3.9 million in 2015, according to University of Michigan researchers. Across all Michigan hospitals, uncompensated care fell by $604 million, consistent with previous findings showing that uncompensated care costs for hospitals in Medicaid expansion states fell by roughly half. [18]
Michigan’s Proposal Would Result in Significant Coverage Loss
Michigan’s waiver proposal would put the gains from Medicaid expansion at risk by making two significant changes to Healthy Michigan. The state proposes to take Medicaid coverage away from enrollees who gained coverage through expansion if they don’t work or engage in other “qualifying” activities for 80 hours each month unless they can show they are exempt.[19] Beneficiaries would have to verify that they’re meeting the state’s new work requirement every month; otherwise they would lose coverage until they complied with the work requirement.[20] The proposal would also more than double premiums, from 2 percent to 5 percent of monthly income, for beneficiaries who have incomes between 100 and 138 percent of the federal poverty line and who have been enrolled in Healthy Michigan for more than 48 consecutive months. Beneficiaries who don’t make their monthly premiums on time would lose coverage after a 60-day grace period and wouldn’t be able to regain their coverage until they come into compliance with the premium requirement. The state’s proposal, however, is unclear whether this means beneficiaries must pay past-due premiums, make a prospective payment, or both.
As noted, the Michigan House Fiscal Agency estimates that up to 54,000 Michiganders would lose Medicaid coverage as a result of the state’s proposal to take Medicaid away from people who don’t meet the work requirement.[21] While troubling, this estimate is likely too low as it excludes coverage losses due to non-payment of premiums, and it also assumes that everyone who is eligible for an exemption from work requirements will secure one when, in reality, many people will likely be stymied by red tape and paperwork.
Work Requirements Would Cause Substantial Numbers to Lose Coverage
Increased red tape would cause many working people and those qualified for an exemption to lose coverage. Many people who should qualify for an exemption likely won’t get one. For example, Medicaid work requirements nationwide would cause disenrollment ranging from 1.4 million to 4 million people among the 23.5 million adults who are under 65 and not receiving Supplemental Security Income based on disability, Kaiser Family Foundation researchers estimated. Most of those losing coverage would be people who are already working or should be exempt.[22]
Evidence from Arkansas also suggests that coverage losses from a work requirement could be even greater than the Michigan House Fiscal Agency’s estimate. Since Arkansas implemented its rigid work requirement in June, over 8,000 Arkansas beneficiaries have lost coverage and are locked out of Medicaid for the rest of 2018 because they didn’t report their work or work-related activities for three months. Over 12,000 others are at risk of losing coverage because they didn’t report in one or two months. Overall, only 2 percent of those required to report satisfied the reporting requirement. [23]
Coverage Losses for Michigan Workers and People With Disabilities, Among Others
In Michigan, three-quarters of Medicaid expansion beneficiaries are working, in school, retired, or unable to work because of a physical or mental impairment.[24] While likely not the intended targets of the policy, people in these groups would be at significant risk of losing coverage:
- Working beneficiaries with unstable jobs. The industries that commonly employ Medicaid enrollees — such as retail, restaurant/food services, home health, and construction — generally feature variable hours, above-average levels of involuntary part-time work and irregular scheduling, and minimal flexibility. This makes it hard for many working people to get the required number of work hours each month to avoid losing coverage.
National data on low-income adults who could be subject to work requirements shows that most work substantial hours over the course of the year, but many do not work consistent hours from month to month as Michigan would require. As a result, 46 percent of low-income workers who could be subject to Medicaid work requirements would be at risk of losing coverage under a 20-hour-per-week requirement. Even among those working 20 hours a week on average over the course of the year, 1 in 4 would be at risk of losing coverage because they do not meet the requirement every month.[25]
- People with disabilities and other vulnerable groups. The Healthy Michigan beneficiary survey found that nearly 70 percent of enrollees have a chronic physical or mental health condition such as diabetes, hypertension, or depression.[26] While the Michigan proposal exempts people who are medically frail or have medical conditions that prevent them from working, some people with disabilities and serious illnesses would inevitably fall through the cracks and lose coverage. This would occur because they don’t meet the criteria for limited exemptions, don’t understand that they do qualify for an exemption, or struggle to provide the documentation proving that they qualify. Bearing out these concerns, studies of state Supplemental Nutrition Assistance Programs and Temporary Assistance for Needy Families (TANF) programs[27] have found that people with disabilities, serious illnesses, and substance use disorders may be disproportionately likely to lose benefits due to work requirements, even when they should be exempt.[28]
- Older Michiganders. Older enrollees also would likely be disproportionately affected. Nationally, nearly two-thirds of Medicaid enrollees potentially subject to work requirements who are under age 50 work, but work rates fall for those over 50, who are more likely to have serious health conditions, and only a minority of 60- to 64-year-old enrollees work.[29] Because the Michigan proposal applies work requirements up to age 62, older adults, including people in their early 60s who decided to retire prior to age 65 because of their health, could lose their health coverage if unable to return to work for 80 hours per month.
Premiums Would Also Cause Coverage Loss
Another provision of Michigan’s proposal would have an even broader reach than the state’s proposed work requirements, putting coverage at risk for parents and students who should be exempt from the work requirement. Almost all adults who have income between 100 and 138 percent of the federal poverty level, and who have been enrolled in Healthy Michigan for 48 consecutive months, would have to pay monthly premiums as high as 5 percent of monthly income. The Medicaid statute prohibits charging premiums to people with incomes below 150 percent of the poverty line, and allowing premiums this high under a waiver would be unprecedented. According to the Michigan House Fiscal Agency, about 35,000 enrollees would now be subject to premiums, and would be in danger of losing their coverage should they miss a payment.[30] People who miss a premium payment would lose coverage for at least one month and could only regain their coverage by coming into compliance with the state’s premium requirement.
Premiums significantly reduce low-income people’s participation in health coverage programs, extensive research shows.[31] The lower a person’s income, the less likely they are to enroll and the more likely they are to drop coverage due to premium obligations. People who lose coverage most often end up uninsured and unable to obtain needed health care services. Evidence from Indiana’s Medicaid waiver shows that premiums have kept large numbers of people from becoming eligible and caused others to lose coverage for non-payment.[32]
Work Requirements Won’t Promote Employment
Studies of work requirements in federal cash assistance programs — TANF and its precursor, Aid to Families with Dependent Children — find that employment increases for those subject to work requirements are generally modest, fade over time, and don’t move many families out of poverty.[33] Cash assistance programs generally provide at least some (albeit inadequate) resources for the supportive services that many low-income adults need to work, such as child care, job training, and transportation assistance. In contrast, the Trump Administration’s Medicaid work requirements guidance says that states imposing these requirements need not offer any new work supports and may not use federal funding for them.[34]
Moreover, even if some enrollees do find jobs because of work requirements, these will probably be mostly low-wage jobs. Such jobs are unlikely to boost enrollees’ incomes enough for them to shift from Medicaid into subsidized individual market coverage, and most of these jobs do not offer affordable health insurance — meaning most enrollees would still need Medicaid. According to Labor Department data, among workers with earnings in the bottom quartile of the wage distribution, only 37 percent are offered health coverage, and less than a quarter actually obtain coverage, presumably in large part because required employee premium contributions are often higher than low-wage workers can afford.[35] Similarly, only 37 percent of full-time workers with family incomes below the poverty line (and only 13 percent of such part-time workers) are even offered coverage.[36] Consistent with these data, in Medicaid expansion states, 42 percent of workers with family incomes below 138 percent of the poverty line obtain health insurance through Medicaid, more than twice the share that obtain insurance through an employer.[37]
Losing coverage and becoming uninsured would have severe adverse impacts on beneficiaries’ physical and financial health. In a 2016 state survey, 83 percent of Healthy Michigan enrollees agreed or strongly agreed that without Medicaid coverage they would not be able to go to the doctor.[38] That’s consistent with a large and growing body of research finding that Medicaid expansion has significantly expanded access to preventive, primary, and other important health care services.[39] Moreover, losing coverage would reverse the recent improvements in physical, mental, and dental health that Healthy Michigan enrollees have reported as a result of coverage.[40] It would also make it harder for beneficiaries to pay their medical bills, and increase the risk of going without needed medical care and incurring significant medical debt for any care they do receive.
Michigan’s Proposal Would Increase State Costs and Uncompensated Care
While noting the difficulty of formulating a precise estimate, the Michigan Senate Fiscal Agency estimates that Michigan would incur between $20 million and $30 million in new administrative costs per year just to implement the new requirements. These costs would go to tracking, verification, and paperwork, as the state doesn’t project any new costs for work supports such as job training, child care, or transportation.
The state’s Senate Fiscal Agency also notes that many people losing Medicaid coverage would end up uninsured but would still seek care, mainly at hospitals, reversing the decline in uncompensated care since Medicaid expansion took effect in April 2014. While the Senate Fiscal Agency does not attempt to quantify the impact on hospital or state uncompensated care costs, the effects could be large. The drop in hospital uncompensated care costs since 2013 amounts to $604 million.
End Notes
[1] State of Michigan, Healthy Michigan Plan Enrollment Statistics as of October 15, 2018, https://www.michigan.gov/mdhhs/0,5885,7-339-71547_2943_66797---,00.html.
[2] Michigan House Fiscal Agency, “Legislative Analysis on Healthy Michigan Work Requirements and Premium Payment Requirements,” June 6, 2018, http://www.legislature.mi.gov/documents/2017-2018/billanalysis/House/pdf/2017-HLA-0897-5CEEF80A.pdf.
[3] Jennifer Wagner, “4,109 More Arkansans Lost Medicaid in October for Not Meeting Rigid Work Requirements,” Center on Budget and Policy Priorities, October 16, 2018, https://www.cbpp.org/blog/4109-more-arkansans-lost-medicaid-in-october-for-not-meeting-rigid-work-requirements.
[4] State of Michigan, “Section 1115 Demonstration Extension Application: Healthy Michigan Plan (Project No. 11-W-00245/5),” September 10, 2018, https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/mi/mi-healthy-michigan-pa3.pdf. Michigan’s Medicaid expansion requires beneficiaries to make monthly payments, which are based on the average co-payments for services used in the previous six months, into a health savings account. In addition to these monthly payments, beneficiaries with incomes between 100 and 138 percent of the poverty level must pay monthly premiums set at 2 percent of their incomes.
[5] For more information on the benefits of Medicaid expansion, see Larisa Antonisse et al., “The Effects of Medicaid Expansion under the ACA: Updated Findings from a Literature Review,” Kaiser Family Foundation, March 28, 2018, https://www.kff.org/medicaid/issue-brief/the-effects-of-medicaid-expansion-under-the-aca-updated-findings-from-a-literature-review-march-2018/, and Government Accountability Office, “Medicaid: Access to Health Care for Low-Income Adults in States with and without Expanded Eligibility,” October 15, 2018, https://www.gao.gov/products/GAO-18-607.
[6] Susan Dorr Goold and Jeffrey Kullgren, “Report on the 2016 Healthy Michigan Voices Enrollee Survey,” University of Michigan Institute for Healthcare Policy & Innovation, January 17, 2018, https://www.michigan.gov/documents/mdhhs/2016_Healthy_Michigan_Voices_Enrollee_Survey_-_Report__Appendices_1.17.18_final_618161_7.pdf.
[7] Institute for Healthcare Policy & Innovation, “Medicaid Expansion Helped Enrollees Do Better at Work or in Job Searches,” University of Michigan, June 27, 2017, http://ihpi.umich.edu/news/medicaid-expansion-helped-enrollees-do-better-work-or-job-searches.
[8] Renuka Tipirneni, Susan D. Goold, and John Z. Ayanian, “Employment Status and Health Characteristics of Adults With Expanded Medicaid Coverage in Michigan,” Journal of the American Medical Association Internal Medicine, April 2018, https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2664514?redirect=true.
[9] Melvin Stephens, Jr., and Desmond J. Toohey, “The Impact of Health on Labor Market Outcomes: Experimental Evidence from MRFIT,” National Bureau of Economic Research Working Paper, January 2018, http://www.nber.org/papers/w24231.
[10] State of Michigan, “Section 1115 Demonstration Extension Application: Healthy Michigan Plan (Project No. 11-W-00245/5).”
[11] Renuka Tipirneni et al., “Primary Care Appointment Availability and Nonphysician Providers One Year After Medicaid Expansion,” American Journal of Managed Care, June 2016, Vol. 22, No. 6, pp. 427-31, https://www.ajmc.com/journals/issue/2016/2016-vol22-n6/primary-care-appointment-availability-and-nonphysician-providers-one-year-after-medicaid-expansion.
[12] State of Michigan, “Section 1115 Demonstration Extension Application: Healthy Michigan Plan (Project No. 11-W-00245/5).”
[13] Eric Charles et al., “Impact of Medicaid Expansion on Cardiac Surgery and Outcomes,” Annals of Thoracic Surgery, October 2017, Vol. 104, No. 4, pp. 1251-1258.
[14] Sarah Miller et al., “The ACA Medicaid Expansion in Michigan and Financial Health,” National Bureau of Economic Research, Working Paper No. 25053, September 2018, http://www.nber.org/papers/w25053.pdf.
[15] Goold and Kullgren.
[16] Michigan House Fiscal Agency, “Healthy Michigan Plan Saving and Cost Estimates,” September 14, 2016, http://www.house.mi.gov/hfa/PDF/HealthandHumanServices/HMP_Savings_and_Cost_Estimates.pdf.
[17] John Z. Ayanian et al., “Economic Effects of Medicaid Expansion in Michigan,” New England Journal of Medicine, February 2, 2017, Vol. 376, No. 5, https://www.nejm.org/doi/full/10.1056/NEJMp1613981.
[18] Thomas Buchmueller et al., “2016 Report on Uncompensated Care and Insurance Rates, December 21, 2017,” https://www.michigan.gov/documents/mdhhs/2013_PA_107_Section_105d8-9_Required_Report_2017_618079_7.pdf; Jessica Schubel and Matt Broaddus, “Uncompensated Care Costs Fell in Nearly Every State as ACA’s Major Coverage Provisions Took Effect,” Center on Budget and Policy Priorities, May 23, 2018, https://www.cbpp.org/research/health/uncompensated-care-costs-fell-in-nearly-every-state-as-acas-major-coverage.
[19] Michigan proposes to exempt the following groups: parents with children under age 6, beneficiaries receiving disability benefits, pregnant women, full-time students, parents or caretakers of family members with a disability, those medically frail, beneficiaries with a medical condition that results in a work limitation (requires medical professional order), beneficiaries who have been incarcerated within the last six months, beneficiaries receiving unemployment benefits, and beneficiaries under age 21 who had previously been in foster care.
[20] Beneficiaries are allowed three months of noncompliance within a 12-month reporting period.
[21] Michigan House Fiscal Agency, “Legislative Analysis on Healthy Michigan Work Requirements and Premium Payment Requirements.”
[22] Rachel Garfield, Robin Rudowitz, and MaryBeth Musumeci, “Implications of a Medicaid Work Requirement: National Estimates of Potential Coverage Losses,” Kaiser Family Foundation, June 27, 2018, https://www.kff.org/medicaid/issue-brief/implications-of-a-medicaid-work-requirement-national-estimates-of-potential-coverage-losses/. To reach their estimates on the impact of work requirements on people who should remain eligible, Kaiser researchers looked at evidence on how administrative requirements affect Medicaid enrollment, which shows that increased red tape causes eligible people to lose coverage. Kaiser researchers applied a low disenrollment rate of 5 percent and a high of 15 percent to the groups of people who are already working or should be exempt based on this evidence.
[23] Wagner, 2018.
[24] Tipireni, Goold, and Ayanian.
[25] For an explanation of the methodology behind these estimates, see Aviva Aron-Dine, Raheem Chaudhry, and Matt Broaddus, “Many Working People Could Lose Coverage Due to Work Requirements,” Center on Budget and Policy Priorities, April 11, 2018, https://www.cbpp.org/research/health/many-working-people-could-lose-health-coverage-due-to-medicaid-work-requirements.
[26] Goold and Kullgren.
[27] LaDonna Pavetti, Michelle Derr, and Heather Hesketh, “Review of Sanction Policies and Research Studies,” Mathematica Policy Research, Inc., March 2003.
[28] For more information on how a Medicaid work requirement would harm specific populations, see https://www.cbpp.org/medicaid-briefs-who-is-harmed-by-work-requirements.
[29] Center on Budget and Policy Priorities, “How Medicaid Work Requirements Will Harm Older Americans,” February 20, 2018, https://www.cbpp.org/research/health/how-medicaid-work-requirements-will-harm-older-americans.
[30] Michigan House Fiscal Agency, “Healthy Michigan Plan Saving and Cost Estimates.”
[31] Samantha Artiga, Petry Ubri, and Julia Zur, “The Effects of Premiums and Cost-Sharing on Low-Income Populations: Updated Review of Research Findings,” Kaiser Family Foundation, June 2017, http://files.kff.org/attachment/Issue-Brief-The-Effects-of-Premiums-and-Cost-Sharing-on-Low-Income-Populations.
[32] The Lewin Group, “Indiana Healthy Indiana Plan 2.0: Interim Evaluation Report,” July 6, 2016, https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/in/Healthy-Indiana-Plan-2/in-healthy-indiana-plan-support-20-interim-evl-rpt-07062016.pdf.
[33] See LaDonna Pavetti, “Work Requirements Don’t Work,” Center on Budget and Policy Priorities, January 10, 2018, https://www.cbpp.org/blog/work-requirements-dont-work; Pavetti, “Work Requirements Don’t Cut Poverty, Evidence Shows,” CBPP, updated June 7, 2016, https://www.cbpp.org/research/poverty-and-inequality/work-requirements-dont-cut-poverty-evidence-shows; and Pavetti, “Evidence Doesn’t Support Claims of Success of TANF Work Requirements,” CBPP, April 3, 2018, https://www.cbpp.org/research/family-income-support/evidence-doesnt-support-claims-of-success-of-tanf-work-requirements. See also Ed Dolan, “Do We Really Want Expanded Work Requirements in Non-Cash Welfare Programs?” Niskanen Center, July 23, 2018, https://niskanencenter.org/blog/expanded-work-requirements-in-non-cash-welfare-programs/.
[34] Centers for Medicare & Medicaid Services letter to state Medicaid directors (18-002), January 11, 2018, https://www.medicaid.gov/federal-policy-guidance/downloads/smd18002.pdf.
[35] Bureau of Labor Statistics, “Healthcare benefits: Access, participation, and take-up rates,” https://www.bls.gov/ncs/ebs/benefits/2017/ownership/civilian/table09a.htm.
[36] Michelle Long et al., “Trends in Employer-Sponsored Insurance Offer and Coverage Rates, 1999-2014,” Kaiser Family Foundation, March 21, 2016, https://www.kff.org/private-insurance/issue-brief/trends-in-employer-sponsored-insurance-offer-and-coverage-rates-1999-2014/.
[37] CBPP calculations from Current Population Survey data for 2016.
[38] Goold and Kullgren.
[39] Hannah Katch, Jennifer Wagner, and Aviva Aron-Dine, “Medicaid Work Requirements Will Reduce Low-Income Families’ Access to Care and Worsen Health Outcomes,” Center on Budget and Policy Priorities, updated August 13, 2018, https://www.cbpp.org/research/health/medicaid-work-requirements-will-reduce-low-income-families-access-to-care-and-worsen.
[40] Goold and Kullgren.
More from the Authors

Areas of Expertise
