Medicaid Block Grant Would Slash Federal Funding, Shift Costs to States, and Leave Millions More Uninsured
If confirmed, President-elect Trump’s nominee for Health and Human Services Secretary — House Budget Committee Chair Tom Price — will be well-placed to advance a proposal that he’s previously supported as part of recent House Republican budget plans to fundamentally change the structure of Medicaid by converting it into a block grant.[1] Trump[2] and House Speaker Paul Ryan[3] also have supported converting Medicaid into a block grant, which would likely eliminate the guarantee that everyone who’s eligible and applies for its benefits would receive them and probably give states sweeping new authority to restrict eligibility, cut benefits, and make it harder for people to enroll. The incoming White House and Republican congressional leaders are reportedly planning to pursue such a block grant in 2017, in addition to repealing the Affordable Care Act (ACA).[4]
A Medicaid block grant would lead to draconian cuts to eligibility, benefits, and provider payment rates.A Medicaid block grant would institute deep cuts to federal funding for state Medicaid programs and threaten benefits for tens of millions of low-income families, senior citizens, and people with disabilities. To compensate for these severe funding cuts, states would likely have no choice but to institute draconian cuts to eligibility, benefits, and provider payments. To illustrate the likely magnitude of these cuts, an analysis from the Urban Institute of an earlier block grant proposal from Speaker Ryan found that between 14 and 21 million people would eventually lose their Medicaid coverage (on top of those losing coverage if policymakers repeal the ACA and its Medicaid expansion) and that already low provider payment rates would be reduced by more than 30 percent.
A block grant would cap federal Medicaid funding in order to achieve savings for the federal government. Under current law, the federal government picks up a fixed percentage of states’ Medicaid costs: about 57 percent, on average (outside of the ACA’s Medicaid expansion). In contrast, under a block grant, states would receive a fixed dollar amount, with states responsible for all Medicaid costs in excess of the cap. Because a Medicaid block grant is explicitly intended to produce significant federal budgetary savings, block grants are designed in ways that give states considerably less federal funding each year than they would receive under the current financing system. That is typically accomplished by basing a state’s initial block grant amount on its current or historical spending and then increasing it annually at a considerably slower rate — such as general inflation — than the currently projected annual growth in federal Medicaid spending. The resulting federal funding cuts would thus grow steadily larger each year.
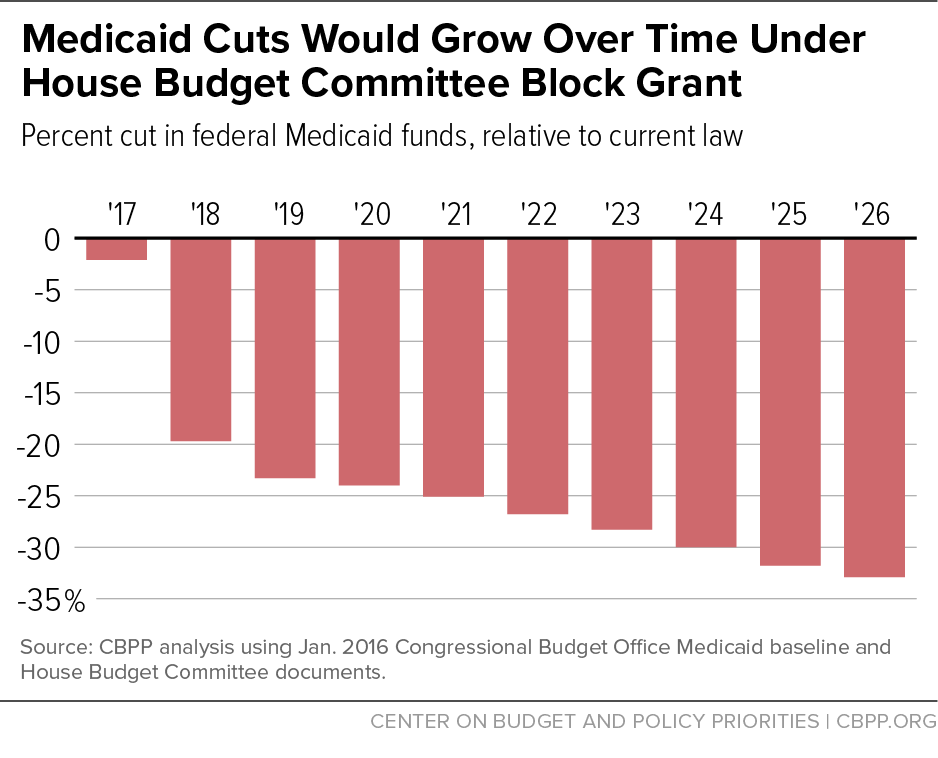
The likely magnitude of the federal funding cuts and resulting cost-shift to states would be very large. The House Republican budget plan for fiscal year 2017, for example, would have cut federal Medicaid funding by $1 trillion — or nearly 25 percent — over ten years, relative to current law, on top of the cuts the plan would secure from repealing the ACA’s Medicaid expansion.[5] By the budget plan’s tenth year (2026), federal funding for Medicaid and the Children’s Health Insurance Program (CHIP) would have been $169 billion — or about 33 percent — less than under current law (see Figure 1). The size of the cuts would have kept growing after 2026.
Moreover, the actual cut in federal funding for states, relative to current law, would be even greater in years when either enrollment or per-beneficiary health care costs rose faster than expected. For example, as people lose their jobs and access to employer-sponsored insurance during a recession, many become newly eligible for and enroll in Medicaid. In addition, developments in new treatments that improve beneficiaries’ health but raise costs, and the onset of epidemics or new illnesses like Zika (or HIV/AIDS in the 1980s), can produce significant unexpected increases in medical costs.[6]
Currently, the federal government and states share in those unanticipated costs. Under a block grant, however, states alone would bear them. Furthermore, while all states would face substantial reductions in federal funding under a block grant, some would likely be hit particularly hard — such as states whose current Medicaid spending levels are already relatively low and states whose spending is expected to rise relatively quickly in future years due to demographic, economic, or other factors.[7]
Such a block grant would push states to cut their Medicaid programs deeply. To compensate for the federal Medicaid funding cuts a block grant would institute, states would either have to contribute much more of their own funding or, as is far more likely, use the greater flexibility the block grant would give them to make draconian cuts to eligibility, benefits, and provider payments. For example, Speaker Ryan’s “Better Way” health plan would give states the choice of a block grant or a Medicaid per capita cap; both would appear to enable states to make sizeable cuts directly affecting beneficiaries that states can’t make now. This could include using waiting lists or capping enrollment; under current law, all eligible individuals who apply for Medicaid must be allowed to enroll. States also could be allowed to no longer provide children with a comprehensive pediatric benefit known as EPSDT (Early Periodic Screening, Diagnostic, and Treatment), under which children enrolled in Medicaid receive both regular check-ups and coverage for all medically necessary treatments that the check-ups find a child needs.
In addition, states could be permitted for the first time to impose a work requirement and terminate coverage for people deemed non-compliant. This could result in people with various serious barriers to employment — such as people with mental health or substance use disorders, people who have difficulty coping with basic tasks or have very limited education or skills, and people without access to child care or transportation — going without health coverage.[8] States would also likely be able to begin charging significant premiums, deductibles, and co-payments at levels that research suggests would likely cause poor people to forgo coverage entirely or go without needed care.
Medicaid is already efficient and innovative. Block grant supporters, including House Republican leaders, often argue that states could compensate for the substantial losses in federal funding they would experience under a block grant by using added flexibility to cut costs without harming beneficiaries. That claim doesn’t withstand scrutiny. Medicaid costs per beneficiary already are far below those of private insurance, after adjusting for differences in health status, due to lower payment rates to health care providers and lower administrative costs, even though Medicaid provides more comprehensive benefits than private insurance at significantly lower out-of-pocket cost to beneficiaries. And over the past three decades, they have also grown much more slowly, on average, than private insurance per-beneficiary costs.[9] They are expected to continue growing more slowly than costs under private insurance in coming years, according to the Medicaid and CHIP Payment and Access Commission.[10]
In addition, states already have substantial flexibility in how they deliver Medicaid services. For example, they have dramatically expanded the use of managed care over the last two decades, instituted cost-containment strategies in areas like prescription drug spending, and in recent years, have adopted numerous innovative reforms in how they deliver care to Medicaid beneficiaries that improve quality of care while lowering costs.[11]
A Medicaid block grant would thus lead to draconian cuts to eligibility, benefits, and provider payment rates. As the Congressional Budget Office concluded in 2012 when analyzing a Medicaid block grant proposal from then-House Budget Committee Chairman Paul Ryan: “the magnitude of the reduction in spending . . . means that states would need to increase their spending on these programs, make considerable cutbacks in them, or both. Cutbacks might involve reduced eligibility, . . . coverage of fewer services, lower payments to providers, or increased cost-sharing by beneficiaries — all of which would reduce access to care.”[12] The Urban Institute estimated that the 2012 Ryan proposal would lead states to drop between 14.3 million and 20.5 million people from Medicaid by the tenth year (in addition to the effects of repealing health reform’s Medicaid expansion).[13] That’s an enrollment decline of 25 to 35 percent. Urban also estimated that the 2012 Ryan block grant would lead states to cut reimbursements to health care providers by more than 30 percent, even though, as noted, provider payments are already much lower than what private insurance and Medicare pays. That could result in many fewer providers and health plans participating in Medicaid, making it far more difficult for beneficiaries to obtain needed care.
End Notes
[1] The past two House Republican budget plans crafted by Rep. Price included a Medicaid block grant, though the fiscal year 2017 budget plan included the option of states electing a “per capita cap” instead. See Edwin Park, “Medicaid Block Grant Would Add Millions to Uninsured and Underinsured,” Center on Budget and Policy Priorities, March 15, 2016, https://www.cbpp.org/blog/medicaid-block-grant-would-add-millions-to-uninsured-and-underinsured and Edwin Park, “Proposed Medicaid Block Grant Would Add Millions to Uninsured and Underinsured,” Center on Budget and Policy Priorities, March 17, 2015, https://www.cbpp.org/blog/proposed-medicaid-block-grant-would-add-millions-to-uninsured-and-underinsured.
[2] See President-elect Donald J. Trump’s campaign website, https://www.donaldjtrump.com/policies/health-care/, accessed November 23, 2016.
[3] As part of his “Better Way” health plan he announced this year, Speaker Ryan proposed to give states the choice of either a Medicaid block grant or a per capita cap. In addition, past budget plans crafted by Speaker Ryan when he was chair of the House Budget Committee included a Medicaid block grant. See Edwin Park and Judith Solomon, “Per Capita Caps or Block Grants Would Lead to Large and Growing Cuts in State Medicaid Programs,” Center on Budget and Policy Priorities, June 22, 2016, https://www.cbpp.org/research/health/per-capita-caps-or-block-grants-would-lead-to-large-and-growing-cuts-in-state and Edwin Park, “Ryan Block Grant Would Cut Medicaid by More than One-Quarter by 2024 and More After That,” April, 4, 2014, https://www.cbpp.org/research/ryan-block-grant-proposal-would-cut-medicaid-by-more-than-one-quarter-by-2024-and-more.
[4] See, for example, Phil Galewitz, “Millions Could Lose Medicaid Coverage under Trump Plan,” Kaiser Health News, November 9, 2016, http://khn.org/news/millions-could-lose-medicaid-coverage-under-trump-plan/.
[5] See Park, op cit.
[6] See, for example, Edwin Park and Matt Broaddus, “Medicaid Block Grant Would Shift Financial Risks and Costs to States,” Center on Budget and Policy Priorities, February 23, 2011, https://www.cbpp.org/research/medicaid-block-grant-would-shift-financial-risks-and-costs-to-states.
[7] See Edwin Park and Matt Broaddus, “Medicaid Block Grant Would Produce Disparate and Inequitable Results Across States,” Center on Budget and Policy Priorities, March 10, 2011, https://www.cbpp.org/research/medicaid-block-grant-would-produce-disparate-and-inequitable-results-across-states and John Holahan and Matthew Buettgens, “Block Grants and Per Capita Caps: The Problem of Funding Disparities among States,” Urban Institute, September 8, 2016, http://www.urban.org/research/publication/block-grants-and-capita-caps.
[8] Hannah Katch, “Medicaid Work Requirement Would Limit Health Care Access Without Significantly Boosting Employment,” Center on Budget and Policy Priorities, July 13, 2016, https://www.cbpp.org/research/health/medicaid-work-requirement-would-limit-health-care-access-without-significantly.
[9] Edwin Park et al., “Frequently Asked Questions About Medicaid,” Center on Budget and Policy Priorities, updated August 10, 2016, https://www.cbpp.org/research/health/frequently-asked-questions-about-medicaid.
[10] Medicaid and CHIP Payment and Access Commission, “Report to Congress on Medicaid and CHIP,” June 2016, https://www.macpac.gov/wp-content/uploads/2016/06/Trends-in-Medicaid-Spending.pdf.
[11] Hannah Katch, “States Are Using Flexibility to Create Successful, Innovative Medicaid Programs,” Center on Budget and Policy Priorities, June 13, 2016, https://www.cbpp.org/research/health/states-are-using-flexibility-to-create-successful-innovative-medicaid-programs.
[12] Congressional Budget Office, “The Long-Term Budgetary Impact of Paths for Federal Revenues and Spending Specified by Chairman Ryan,” March 2012, http://www.cbo.gov/sites/default/files/cbofiles/attachments/03-20-Ryan_Specified_Paths_2.pdf.
[13] John Holahan et al., “National and State-by-State Impact of the 2012 House Republican Budget Plan for Medicaid,” Kaiser Commission on Medicaid and the Uninsured, October 1, 2012, http://kff.org/health-reform/report/national-and-state-by-state-impact-of/.
More from the Authors
