Harsh Tradeoff at Core of GOP Health Bill: Keep Medicaid Expansion or Cut Taxes for Wealthy?
Tax Cuts for 400 Highest-Income Households Exceed Cost of Maintaining Expansion in Most States
The House-passed bill to repeal and replace the Affordable Care Act (ACA), which the emerging Senate Republican health bill is expected to largely resemble, would lavish tax cuts on the wealthy and pay for them by cutting provisions that help millions of people afford health coverage and care.[1] New state-by-state estimates from the Urban Institute on the impact of ending the ACA’s Medicaid expansion in the 31 states and the District of Columbia that have adopted it make the tradeoffs at the heart of the GOP health bill even clearer.[2] Using those estimates combined with Joint Committee on Taxation and Tax Policy Center estimates of the impact of the bill’s tax cuts, we find:
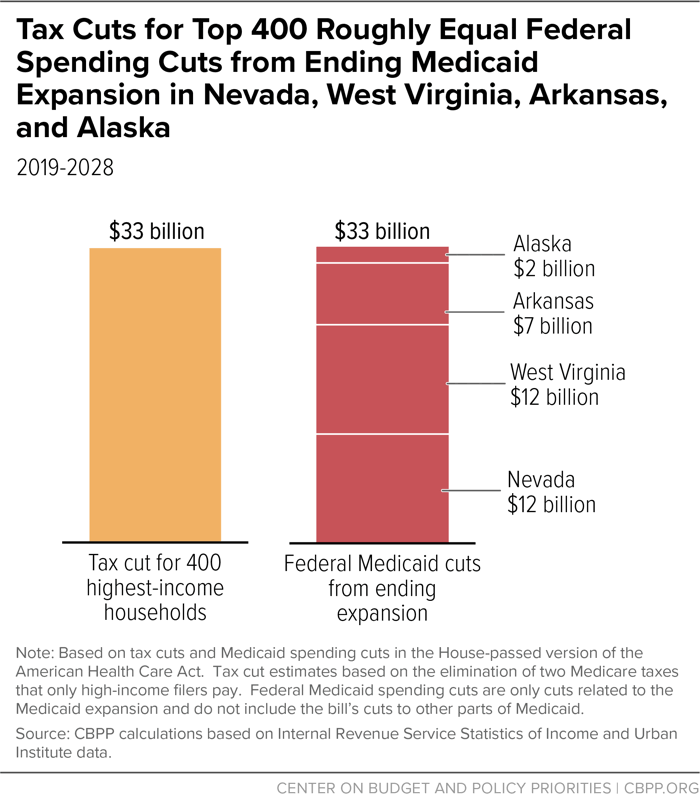
- Households with incomes above $1 million a year would get annual tax cuts averaging more than $50,000 apiece — worth more than the cost of continuing Medicaid expansion coverage for eight people.The 400 highest-income taxpayers alone would receive tax cuts worth about $33 billion from 2019 through 2028, which is more than the federal spending cuts from ending the Medicaid expansion in any one of 20 expansion states and the District of Columbia. In fact, the tax cuts for the top 400 roughly equal the federal cost of maintaining the expansion in Nevada, West Virginia, Arkansas, and Alaska combined. (See Figure 1.) Policymakers face a stark choice: maintain the Medicaid expansion coverage for 726,000 people in these four states, or advance the pending legislation and cut taxes by millions of dollars a year for 400 households whose annual incomes average more than $300 million apiece.
- Households with incomes above $1 million a year would get annual tax cuts averaging more than $50,000 apiece — worth more than the cost of continuing Medicaid expansion coverage for eight people.[3]
GOP Bill: Large Tax Cuts for Wealthy, Damaging Cuts to Medicaid
In its fundamental structure, the House-passed bill cuts taxes for the wealthy and corporations and pays for it by cutting provisions that help millions of people afford health coverage and care. The bill would effectively end the ACA’s Medicaid expansion for low-income adults; cap and cut federal Medicaid funding for seniors, people with disabilities, and families with children; and slash subsidies that help moderate-income people afford individual market insurance coverage. In this analysis, we specifically compare the bill’s tax cuts and the cost of maintaining current federal funding for the Medicaid expansion.
The House-passed bill eliminates the ACA’s enhanced federal match rate for new enrollees under the Medicaid expansion starting in 2020, meaning that states would have to pay three to five times as much for new enrollees as under current law. The large increase in costs would lead most or all states to close their expansions to new enrollees and, since the overwhelming majority of current enrollees would leave Medicaid within a few years, the House bill would effectively end the expansion. The emerging Senate health bill will reportedly phase down federal funding for the expansion over several years, but it would produce the exact same result over time: the Medicaid expansion’s demise.[4]
The Urban Institute estimates that, if states end their expansions starting in 2020, the federal government would save about $700 billion from 2019 through 2028 from lower spending in current expansion states, and 12 million newly eligible people in these states would lose coverage. (The 12 million figure does not include the additional several million people that the Urban Institute estimates could lose coverage due to the federal funding cuts from the GOP bill’s caps on per-enrollee federal Medicaid funding.)[5]
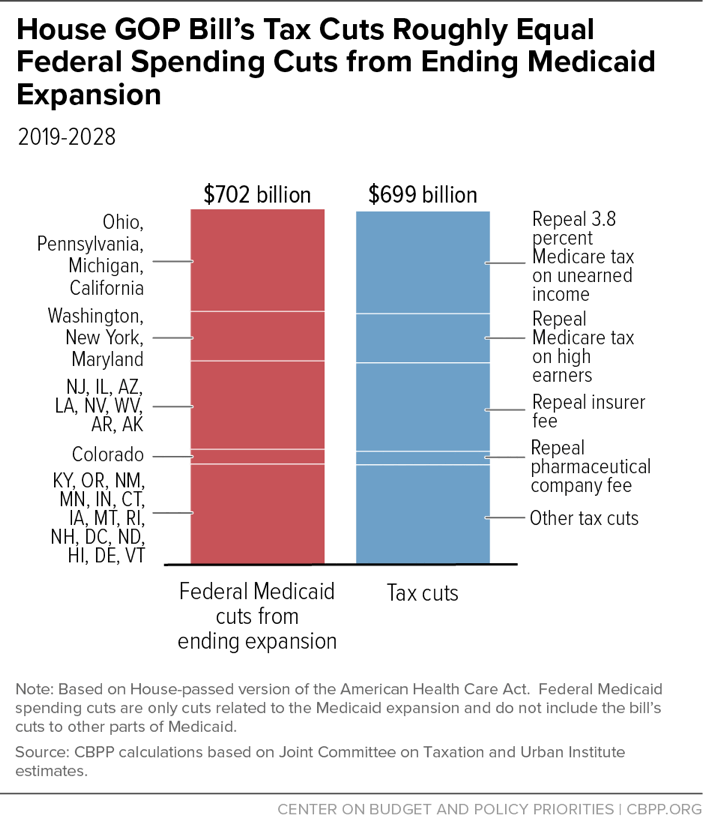
Meanwhile, the House-passed bill would spend about $700 billion from 2019 through 2028 on tax cuts mainly for high-income people and wealthy corporations from repealing the ACA taxes that fall on them, we estimate based on Joint Committee on Taxation data.[6] The repealed taxes would include the ACA’s two so-called Medicare taxes — the additional 0.9 percent Hospital Insurance payroll tax on high-income people and the 3.8 percent tax on unearned income — that fall only on individuals with incomes above $200,000 ($250,000 for married couples), as well as fees that insurance and drug companies pay.[7] (See Figure 2 and Appendix Table 1 for a comparison of the Medicaid spending cuts by state with the tax cuts under the House bill.)
These tax cuts would flow largely to the wealthy and corporations. Households with incomes above $1 million would receive nearly half of the tax cuts, with their tax cuts averaging more than $50,000 apiece each year once they’re fully in effect.[8] Those at the very top would receive even bigger tax cuts. The 400 highest-income households — whose incomes average more than $300 million a year — would get annual tax cuts averaging millions of dollars each. These households would receive total tax cuts worth roughly $33 billion over ten years, we estimate.[9] The value of the tax cuts for the top 400 exceed the federal spending cuts from ending the Medicaid expansion in any one of 20 expansion states and the District of Columbia under the House bill. Indeed, the tax cuts for the top 400 alone roughly equal the federal spending cuts from ending the Medicaid expansion in Nevada, West Virginia, Arkansas, and Alaska combined. Ending expansion in these four states would lead 726,000 people in those states to lose Medicaid coverage.[10]
These estimates reveal misplaced priorities in the Republican approach to health reform, and the harsh consequences for millions of people if the policies are enacted.
| APPENDIX TABLE 1 | ||||
|---|---|---|---|---|
| Appendix: Federal Spending Cuts from Repealing Medicaid Expansion and Tax Cuts in House-Passed Bill (2019-2028) | ||||
| Medicaid Spending Cuts (in billions) | Tax Cuts (in billions) | |||
| State | Cuts (billions) | Provision | Cost (billions) | |
| California | $74.3 | Repeal 3.8% Medicare tax on unearned income | $202 | |
| New Jersey | $59.0 | |||
| Ohio | $50.8 | Repeal 0.9% Medicare tax on high earners | $97 | |
| Kentucky | $45.2 | |||
| Michigan | $41.9 | Repeal insurer fee | $174 | |
| Illinois | $40.2 | Repeal "Cadillac" tax on high-cost health plans | $66 | |
| Oregon | $37.5 | |||
| Washington | $37.5 | Reduce medical expense deduction threshold to 7.5% | $44 | |
| New York | $35.9 | |||
| Pennsylvania | $34.8 | Repeal pharmaceutical company fee | $27 | |
| Colorado | $28.9 | |||
| New Mexico | $27.2 | Repeal medical device tax | $24 | |
| Maryland | $24.5 | Repeal reduced flexible spending account contribution limits | $29 | |
| Arizona | $24.0 | |||
| Minnesota | $20.2 | Increase Health Savings Account limits and other changes | $24 | |
| Indiana | $20.1 | |||
| Louisiana | $18.2 | Repeal other tax changes | $11 | |
| Nevada | $12.2 | |||
| West Virginia | $12.2 | |||
| Connecticut | $12.1 | |||
| Iowa | $7.3 | |||
| Arkansas | $6.9 | |||
| Montana | $6.2 | |||
| Rhode Island | $5.9 | |||
| New Hampshire | $4.7 | |||
| District of Columbia | $3.4 | |||
| North Dakota | $2.8 | |||
| Hawaii | $2.6 | |||
| Delaware | $2.4 | |||
| Alaska | $1.9 | |||
| Vermont | $1.6 | |||
| Total | $702 | Total | $699 | |
End Notes
[1] Chye-Ching Huang and Brandon DeBot, “House Health Bill: Tax Cuts for Wealthy, Insurers, and Drug Companies Paid for by Low- and Middle-Income Families,” Center on Budget and Policy Priorities, May 22, 2017, https://www.cbpp.org/research/federal-tax/house-health-bill-tax-cuts-for-wealthy-insurers-and-drug-companies-paid-for-by.
[2] John Holahan et al., “The Impact of the AHCA on Federal and State Medicaid Spending and Medicaid Coverage: An Update,” Urban Institute, June 16, 2017, http://www.urban.org/research/publication/impact-ahca-federal-and-state-medicaid-spending-and-medicaid-coverage-update.
[3] CBPP calculation for 2025 based on Urban Institute data and Tax Policy Center (TPC) tables T16-0295, and T16-0315.
[4] Matt Broaddus and Edwin Park, “House Republican Health Bill Would Effectively End ACA Medicaid Expansion,” Center on Budget and Policy Priorities, June 6, 2017, https://www.cbpp.org/research/health/house-republican-health-bill-would-effectively-end-aca-medicaid-expansion.
[5] Holahan et al., 2017.
[6] CBPP analysis based on JCX-27-17 cost estimates for 2017-2026. We estimate the cost of individual provisions through 2028 by assuming that the cost continues to change by the same amount as it does between 2025 and 2026. We assume that the “Cadillac tax” on high-cost health plans remains in place after 2026 as it would under the House bill. The estimate does not include the reported “reserve fund” from dropping the medical expense deduction threshold further from 7.5 percent to 5.8 percent, or proposed changes to coverage provisions (including the premium tax credit and the individual and employer mandates). Joint Committee on Taxation, “JCX-27-17: Estimated Revenue Effects Of The Tax Provisions Contained In Title II Of H.R. 1628, The ‘America Health Care Act Of 2017,’ As Passed By The House Of Representatives,” May 24, 2017, https://www.jct.gov/publications.html?func=startdown&id=5000.
[7] For more on the tax cuts in the House GOP health bill, see Huang and DeBot, 2017.
[8] TPC tables T16-0295 and T16-0315. The estimate includes the repeal of the following revenue-raising provisions as modeled by TPC: the 3.8 percent net investment income tax on unearned income, the 0.9 percent additional Hospital Insurance tax, the increase in the threshold for medical expense deductions, the “Cadillac tax” on high-cost health plans, and the excise taxes on insurers, pharmaceutical manufacturers and importers, and medical device manufacturers and importers. It does not include the proposed changes to coverage provisions (including the premium tax credit and the individual and employer mandates).
[9] CBPP estimate for the tax cuts from repeal of two Medicare taxes that only high-income households pay, based on Internal Revenue Service Statistics of Income data for 2014. For detailed methodology, see Brandon DeBot, Chye-Ching Huang, and Chuck Marr, “ACA Repeal Would Lavish Medicare Tax Cuts on 400 Highest-Income Households,” Center on Budget and Policy Priorities, January 12, 2017, http://bit.ly/2jzK2uI. We update the estimate in that paper to take into account the delay of the repeal of the 0.9 percent additional Medicare Hospital Insurance tax to 2023 in the final House bill, and the fact that the tax cuts would likely grow over time as incomes for those at the top increase (specifically, we assume that these tax cuts grow at the same rate as the overall revenue loss from repealing the Medicare taxes).
[10] Holahan et al., 2017.
