Everyone needs safe, decent, stable housing. For some of the most vulnerable people in America — people with mental illness, chronic health conditions, histories of trauma, and other struggles — a home helps them to get adequate treatment and start on the path toward recovery. But some conditions make it difficult for people to maintain a stable home without additional help. Supportive housing, a highly effective strategy that combines affordable housing with intensive coordinated services, can provide that needed assistance.
Living without stable housing can drastically worsen health. Homelessness can exacerbate mental illness, make ending substance abuse difficult, and prevent chronic physical health conditions from being addressed. People with these and other health issues often end up in crisis situations while living on the streets, and emergency rooms may be the only health care they are able to access.
Although affordable housing is part of the solution, some people may need their housing coupled with supportive services to maintain it. For instance, service providers can help people with mental illness pay their rent on time and understand the rights and responsibilities outlined in a lease, or can make sure people with chronic illnesses manage their diet and medicine properly, which can keep them out of hospitals or nursing homes.
A broad body of research shows that supportive housing effectively helps people with disabilities maintain stable housing. People in supportive housing use costly systems like emergency health services less frequently and are less likely to be incarcerated. Supportive housing also can aid people with disabilities in getting better health care and help seniors trying to stay in the community as they age and families trying to keep their children out of foster care.
Policymakers, administrators, and health providers are increasingly aware that a lack of stable housing can interfere with health goals, and that linking health care with affordable housing can produce better outcomes for some people than providing them separately. Yet there is not nearly enough supportive housing to meet the need. Policymakers can create additional supportive housing by:
- Providing additional rental assistance and other housing resources;
- Reinvesting savings created by supportive housing that reduces use of health services and corrections to increase the supply of rental assistance;
- Making greater use of Medicaid services for supportive housing; and
- Targeting supportive housing only on those who need it.
Essential Characteristics of Supportive Housing
Supportive housing is a highly effective strategy that combines affordable housing with intensive coordinated services to help people struggling with chronic physical and mental health issues maintain stable housing and receive appropriate health care. Supportive housing features:
Permanence and affordability. Tenants generally pay no more than 30 percent of their income for rent. They have the same rights and responsibilities as other renters, such as having the lease in their name and the right to privacy in their unit, which means they cannot be evicted for reasons unrelated to being a good tenant.
A core set of service principles. They are:
- Services are housing-oriented. Services aim to help tenants remain housed. Service providers help people find suitable housing, build relationships with their landlords, and understand their rights and responsibilities as renters. Providers also intervene to prevent evictions.
- Services are multi-disciplinary. Service providers also help tenants address physical health, mental health, and substance use conditions, and help with other issues like applying for Social Security benefits or gaining employment. Teams of professionals such as mental health and substance use specialists, nurses or doctors, and case managers provide care. Services must be flexible enough to address each individual tenant's needs, which may involve multiple service agencies working together. These teams also try to link people to mainstream service systems like work training, if appropriate
- Services are voluntary but assertive. Services are voluntary; tenants will not lose their housing simply because they do not participate in services. But providers offer supportive services assertively, which means that they will continue to show up and check on someone even if tenants don’t request help.
Integration. Individuals and families are able to live independently in apartments or single-family homes in residential neighborhoods. Tenants in supportive housing should have access to public transportation, grocery stores, parks, and other neighborhood amenities common to all other residents. Services are usually provided in the client’s unit or building, or at a place of their choosing in the community, and clients should not lose access to services if they choose to live somewhere else. (Less accessible services put tenants’ housing and health at risk: if they are unable to travel to providers’ offices, for instance, they may stop using the services.)
Emphasis on choice. Supportive housing maximizes client choice, in clients’ housing options and the services they receive. For instance, tenants can generally come and go as they please and have control over their daily schedule, like mealtimes and visitors. They also can direct the types of services they receive and the goals they set with the service provider.
Low barriers to entry. Supportive housing providers do not require clients to hit benchmarks before moving into housing or put other screening barriers in the way. Blanket bans on people with criminal histories or bad credit, for example, or requirements to meet goals, like employment or completing a course of treatment, before entering supportive housing would screen out the very people supportive housing aims to help.
Other models combine housing and services but are not supportive housing, although the lines between models are not always bright. Nursing homes, for instance, restrict residents’ choice and do not allow them to live in the community. Other models use affordable housing as a platform to improve residents’ health and quality of life — often called “service-enriched housing” — but the services they provide, like in-home nutrition classes for the elderly, are not necessary for residents to maintain stable housing.
Evidence Backs Supportive Housing
A large body of research shows that the vast majority of people who live in supportive housing are able to stay stably housed in the community. Research has also examined the effect of supportive housing on other outcomes, like mental and physical health, and the use of health care systems, corrections, and other systems.
Most of this research focuses on people with severe disabilities experiencing homelessness, especially people with mental illness or substance use disorders as well as other chronic physical health issues like HIV/AIDS.[2] A few more recent studies evaluate supportive housing for other groups, such as seniors and families.
The research supports four main conclusions:
- Supportive housing helps people with disabilities live stably in the community.
- People with disabilities in supportive housing reduce their use of costly systems, especially emergency health care and corrections.
- Supportive housing can help people with disabilities receive more appropriate health care and may improve their health.
- People in other groups, including seniors trying to stay in the community as they age and families trying to keep their children out of foster care, likely also benefit from supportive housing.
Building on this strong body of research, supportive housing practice is expanding to help other vulnerable people, such as homeless youth,[3] who often have spent time in the foster care system and struggle with mental health issues and trauma, and people with developmental disabilities, who often live in segregated group homes rather than being integrated into the community. The existing research suggests that supportive housing would be successful for such other groups, but researchers should continue to examine how supportive housing’s impact might differ for them.
Supportive Housing Helps People With Disabilities Live Stably in the Community
In studies conducted of this population, at least 75 percent of homeless people with mental illness or other serious disabilities (including those who have been homeless for long periods) who entered supportive housing as part of such a study remained through the study’s end (usually 18 to 24 months). Although few studies have followed tenants for much longer, of those that have, at least half of the tenants stayed for as long as five years.[4]
Supportive housing achieves much better housing stability than case management without rental assistance.[5] Tenant housing stability in supportive housing is similar to stability in more segregated housing and service models like group homes and nursing homes, but tenants highly prefer supportive housing.[6] The success seems to hold for a range of disabilities — people with physical disabilities or chronic illnesses such as HIV/AIDS fare well in supportive housing,[7] as do people with severe mental illness or substance abuse disorders.[8]
People with disabilities who lived in supportive housing after release from jail or prison were 61 percent less likely to be re-incarcerated one year later than those not offered supportive housing.People with mental illness and other severe disabilities are also more likely than others to be incarcerated or to enter long-term health care institutions like nursing homes or psychiatric hospitals, or to cycle between institutionalization and homelessness.[9] Many studies show that supportive housing successfully interrupts this cycle — people with histories of incarceration or institutionalization significantly reduce their use of those systems after moving into supportive housing. One of the largest studies to date that documents these reductions, conducted in New York City, found that individuals placed in supportive housing spent, on average, 115 fewer days per person in homeless shelters, 75 fewer days in state-run psychiatric hospitals, and almost eight fewer days in prison or in jails, in the two years after entering supportive housing, compared to a similar group without supportive housing.[10]
Most studies recruit people from homeless shelters or off the streets, but a few small studies use supportive housing to help people move out of nursing homes or other institutions.[11] One found that a group in supportive housing recruited from psychiatric hospitals moved quickly out of the institutions and avoided subsequent homelessness, while a group without supportive housing exited institutions much more slowly and experienced more homelessness two years later.[12]
The research on supportive housing designed to move people with disabilities directly out of jails or prisons is limited to a few studies, most of which are case studies. One of the most recent and well designed tracked 121 participants who lived in supportive housing after release and 118 who did not. Those in supportive housing were 43 percent less likely to be rearrested on misdemeanor charges (though there was no difference in the likelihood of felony arrests), and were 61 percent less likely to be re-incarcerated one year later.[13]
Supportive Housing Reduces the Use of Other Costly Systems
Many researchers and policymakers are now trying to understand to what extent associated reductions in the use of homeless shelters, prisons and jails, and health care — including emergency room visits, inpatient hospitalizations, and stays in nursing homes or psychiatric hospitals — can offset the cost of supportive housing.
The results of the existing studies vary somewhat in the magnitude of the cost reductions and the particular systems affected. One of the larger studies found reductions mostly in the homelessness system,[14] while a number of others found reductions across multiple systems like the study in New York, referenced above, in which use reductions offset about 95 percent of the cost of the supportive housing.
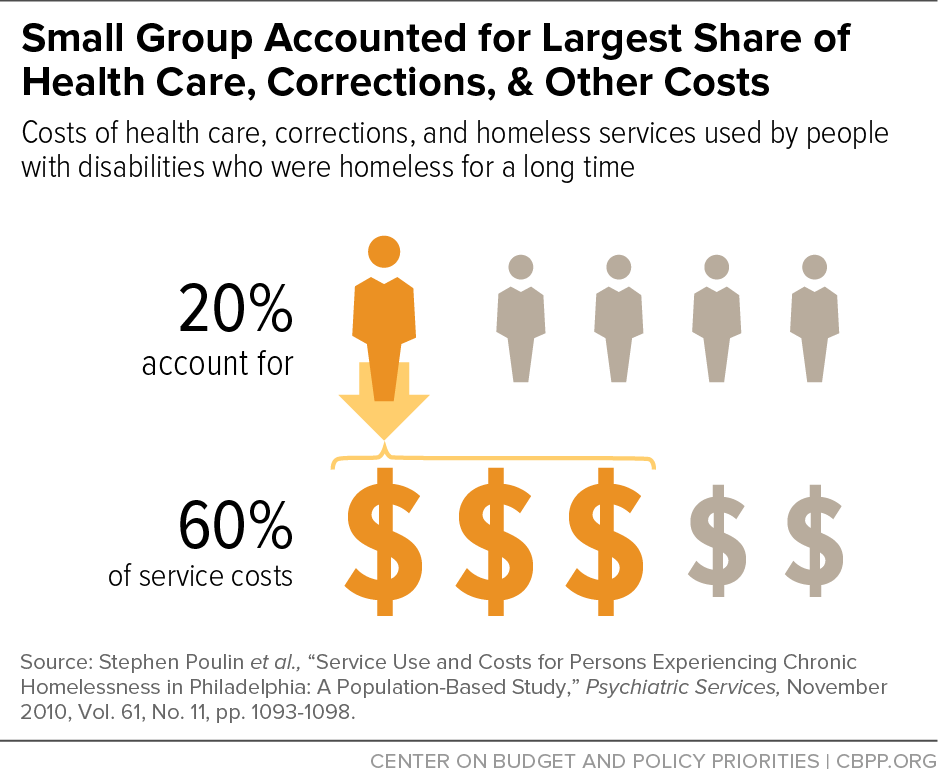
The evidence suggests that the greatest reductions are likely achieved with supportive housing that focuses on people who are the costliest utilizers of services. People experiencing homelessness are not homogenous: a study in Philadelphia that tracked the costs of services used by people with disabilities who were homeless for a long time found that about 20 percent of that group accounted for 60 percent of the health care, corrections, and homeless services costs (see Figure 1).[15] Targeting less frequent users may not significantly impact other systems or save money.
A large-scale study in Canada compared high- and moderate-need groups of homeless individuals with mental illness.[16] Two years after they were offered supportive housing, both groups had high rates of stable housing, but only the high-needs group reduced use of health care and corrections systems. The moderate-need group actually increased its use of health care, likely because supportive housing provided better access to appropriate health services.[17] (Other studies have shown similar increases in outpatient services after entering supportive housing.)
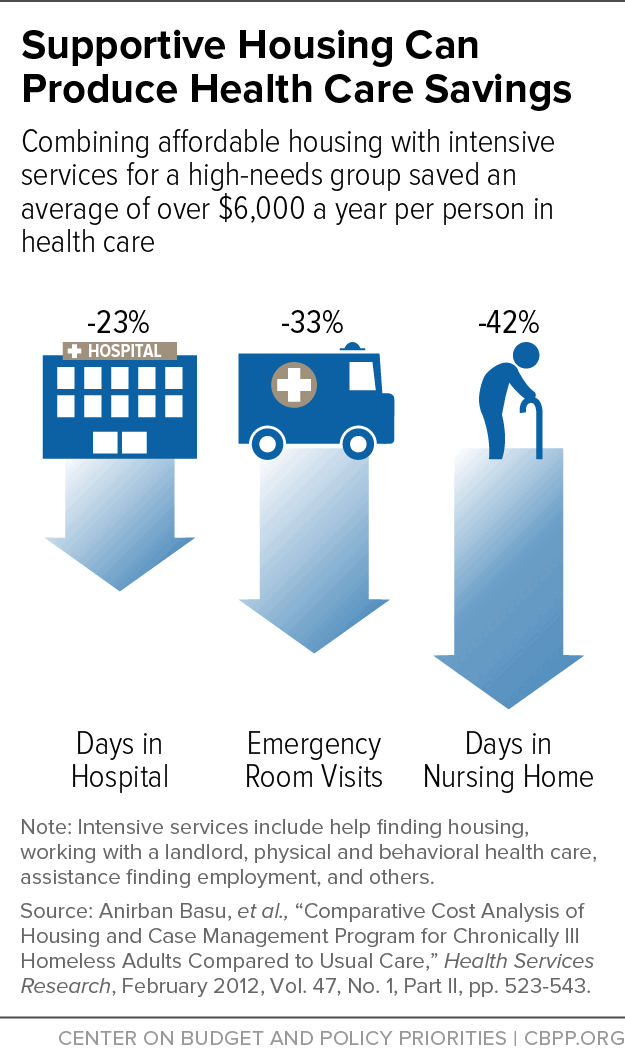
One well-designed study targeted a particularly high-needs group and found that savings in the health care system could be substantial.[18] The study recruited homeless, hospitalized people with chronic illnesses that have a high risk of mortality. On average, people offered supportive housing spent 23 percent fewer days in hospitals, had 33 percent fewer emergency room visits, and spent 42 percent fewer days in nursing homes, per year during the study period, among other positive results.[19] The study estimated that these reductions (and others) more than offset the cost of supportive housing, resulting in over $6,000 in annual savings per person (see Figure 2). Although this study focused on a very specific population — so working with a different group may not produce similar results — it illustrates the potential cost savings of providing a high-needs group with supportive housing.
Promising Findings Suggest Supportive Housing May Improve Health
Supportive housing helps people get appropriate care for their health conditions by reducing use of emergency health services and increasing use of outpatient services. Due to a focus on housing stability as supportive housing’s primary goal, there have not been many studies on the mental or physical health outcomes (such as improved diabetes management, lower blood pressure, and controlled chronic conditions) of people in supportive housing. More high-quality research on health outcomes is needed.
The strongest findings in this area show that supportive housing reduces the risk of death among the small subset of people with HIV/AIDS, and may also lessen the amount of the virus in their bloodstream.[20] In a separate analysis of the high-needs group study referenced above, participants with HIV/AIDS in supportive housing were 63 percent more likely to be alive and have an intact immune system — a measure of disease progression — than those in the control group.[21] Other studies have found similar increases in survival among people with HIV/AIDS in supportive housing.[22]
Few supportive housing studies track mental health outcomes. A few more track substance use, but only a handful compare groups with and without supportive housing.[23] Among those that use comparison groups, some find that people in supportive housing do not differ in their substance use from those who are not in supportive housing,[24] but one notable study found large reductions in alcohol and other drug use after homeless veterans were randomly assigned to receive supportive housing.[25]
Getting an accurate picture of substance use, especially among the groups without supportive housing, is extremely difficult for a number of reasons, especially the unreliability of self-reports of drug use and low response rates to follow-up among those without supportive housing. The study that found reductions in substance use is the only one that specifically adjusted for these differential follow-up rates. [26]
“… participants with HIV/AIDS in supportive housing were 63 percent more likely to be alive and have an intact immune system.”A majority of the evidence on behavioral health in supportive housing simply compares substance use and mental health symptoms before and after entering supportive housing (rather than using comparison groups). These studies show consistently that those in supportive housing reduce their use of substances over time, and at least one study shows a reduction in mental health symptoms as well.[27] Together the available studies indicate that supportive housing works at least as well as other treatments available in the community to help people experiencing homelessness reduce their substance use and may be more effective.
Clearly, more high-quality research is needed, especially research that examines the type of mental health and substance use services that are widely used in supportive housing. For example, there is strong evidence that a treatment model called Assertive Community Treatment (ACT) reduces psychiatric symptoms and increases housing stability for people with severe mental illness who are experiencing homelessness,[28] and a technique called Motivational Interviewing (MI) has been shown to reduce drug and alcohol use.[29] Yet no supportive housing study specifically tests the effect of different behavioral health treatment models. There is no reason to believe that ACT, MI, or other evidence-based treatment models would be less effective in stable housing, but researchers should evaluate whether different treatments could be more effective when administered as part of supportive housing.
Other Groups Can Benefit From Supportive Housing
Additional limited research shows that supportive housing is a promising model for helping people in other groups, including seniors trying to stay in the community as they age and families trying to keep their children out of foster care.
Model Likely Can Help Frail Seniors Age in the Community
Some homeless people with severe disabilities are elderly.[30] But other seniors who have never needed support before may find it difficult to stay in their homes as their health worsens. Supportive housing can likely help these seniors avoid or delay entry into nursing homes and other care facilities, although only a few studies have examined the use of supportive housing for this purpose.
One study provided supportive housing to seniors already living in affordable housing and compared their rates of nursing home admission and hospitalization to seniors in affordable housing in the same community without supportive housing.[31] Seniors in buildings in which supportive housing was offered were half as likely to enter nursing homes as seniors in the buildings without supportive services.[32] Individuals with supportive housing were also much less likely to go to the hospital. This is consistent with broader health care research that finds that in-home support for seniors can effectively reduce their rate of admission to nursing homes.[33]
Supportive Housing Can Help Keep Families Together
Many families with children struggle with severe disabilities and homelessness. The few supportive housing studies that include families show results similar to those for homeless individuals.[34]
The Building Blocks of Supportive Housing
Supportive housing is created from rental assistance, services, and in some cases, development funding (see appendix for a list of federal funding sources).
Rental Assistance
Low-income households usually cannot afford market-rate rents, and the rents they can afford don’t cover owners’ costs of operating and maintaining the housing. Rental assistance fills that gap: tenants usually pay 30 percent of household income for rent, and the rental assistance covers the rest.
Rental assistance comes in two forms: tenant-based and project-based. Households with tenant-based rental assistance select a privately owned unit. The assistance moves with them if they relocate, which may enable them to move close to family, service providers, or jobs. Project-based rental assistance is attached to specific apartments by contract, and the subsidy stays with the unit if the tenant moves. Attaching project-based rental assistance to multiple supportive housing units in a building allows service providers to deliver services more efficiently. Project-based contracts can also help owners finance new developments or rehabilitate properties.
Services
Supportive services funding is usually cobbled together from multiple federal, state, and local grants. Federal funding is often restricted to specific groups. For instance, the Substance Abuse and Mental Health Services Administration funds services for people with mental health and substance use disorders, the Administration for Children and Families programs can support family stability, and the Department of Veterans Affairs provides health care for veterans.
Medicaid provides health insurance coverage to low-income families and individuals and is designed to be a stable funding source for health care. Medicaid is available to everyone who qualifies — in contrast with the programs above, which are constrained by set funding levels — and can provide a broad range of services and supports. But not all states provide supportive housing-related health services through Medicaid.
Development
Many supportive housing providers rely on existing private market housing, which tenants can lease with the help of rental assistance. But some supportive housing providers develop and operate their own properties, which requires funding to acquire, build, or rehabilitate the housing. Developing supportive housing enables providers to configure the space to accommodate on-site services and their tenants’ needs, and development is important in markets where there is little available rental housing, such as high-cost urban areas and some rural areas.
Grants and other development subsidies are used in many projects to reduce the amount that a developer must borrow to finance the development, which allows the owner to offer lower rents, since less rental income is needed to cover the owner’s loan costs. However, even if the owner of a development has no outstanding debt on the property, rental assistance is usually necessary to cover owners’ regular maintenance and administrative costs.
Keeping a family intact while struggling with homelessness and mental illness is difficult. Separation is very common for homeless families: children in families experiencing homelessness often live separately from their parents, and they have an elevated risk of involvement with the child welfare system.[35] Affordable housing alone would enable many homeless families to remain together: a recent major study showed that children in homeless families offered rental assistance, with no additional services provided, had fewer placements in foster care.[36]
A small group of families likely needs supportive housing to stay intact. Similar to single adults who are frequent users of health care and correctional systems, a subgroup of families are frequent users of the child welfare system. Research on these families indicates that they have higher rates of mental health and substance use issues, and they experience long-term financial instability that severely limits their ability to pay for rent, heat, food, health care, and other essentials.[37]
The Keeping Families Together demonstration examined supportive housing targeted on families that were involved in the child welfare system and had other service needs. The study began as a small pilot project in New York City that served 29 child welfare-involved families that had been homeless for long periods of time and had a parent with a disabling condition. The families had been homeless for at least ten months (and for up to 12 years), and almost all struggled with mental illness or a history of substance use. About half of the families had two or more child welfare cases in the three years prior to moving into supportive housing, and less than half of the children in these families were living with their birth parents at the time of move-in. Over 60 percent of the child welfare cases that were open when families moved in were subsequently successfully closed, all of the children who were in foster care with a goal of reunification were reunited with their families, and reports of child abuse or neglect dropped from an average of 2.1 incidents per family to 0.6 incidents per family after moving into supportive housing.[38] The Department of Health and Human Services is implementing and testing a five-site demonstration to expand this model.[39]
Bringing Supportive Housing to Scale
Despite its effectiveness, few of the people who would benefit most from supportive housing actually receive it. There are no exact estimates of either the need for or supply of supportive housing, though there are some good data on homelessness.[40] To meet the need, policymakers should consider four interrelated strategies to expand supportive housing:
- Provide additional rental assistance and development resources;
- Reinvest savings created by supportive housing to add to the stock of rental assistance;
- Increase the use of Medicaid services for supportive housing; and
- Target supportive housing only on those who need it.
Expanding Rental Assistance and Supportive Housing Development
Most rental assistance is federally funded, yet only one in four eligible low-income households receives assistance.[41] Expanding available rental assistance is essential to meeting the need for supportive housing. A number of options are available to federal, state, and local policymakers to expand rental assistance.
- Expand the Housing Choice Voucher program. Vouchers used for supportive housing have played a major role in reducing veterans’ homelessness in recent years.[42] Additional housing vouchers could play a critical role in bringing supportive housing to scale to help other needy individuals and families. Vouchers are the only major form of federal rental assistance that can be expanded to serve more households[43] and are particularly well-suited for supportive housing. Housing Choice Vouchers can be tenant-based or project-based,[44] allowing communities flexibility over how they implement supportive housing. Unlike other project-based rental assistance, project-based vouchers allow tenants to move out of the unit with an available tenant-based voucher after one year (while the subsidy stays with the unit). This ensures that tenants do not risk losing housing assistance if they wish to live somewhere else and allows tenants to move out of supportive housing if they no longer need it (more on this below). Policymakers could encourage public housing agencies to use a portion of new vouchers for supportive housing where needed.
- Expand smaller federal programs that provide rental assistance to special populations. A number of smaller programs provide rental assistance to certain groups such as people experiencing homelessness, seniors, non-elderly people with disabilities, and people living with HIV/AIDS (see appendix for a list of federal rental assistance programs and the people served by each program). Recent increases in supportive housing for the chronically homeless, mainly through McKinney-Vento Homeless Assistance Grants, which provide long-term rental assistance for supportive housing, have helped drive a 30 percent decline in chronic homelessness since 2007.[45] Programs targeting other populations can provide supportive housing if properly targeted and combined with services.
- States could fund additional rental assistance. Massachusetts, for instance, funds supportive housing for about 1,300 households. At least 34 states have at least one program that provides housing assistance to low-income people, which often are used for supportive housing.[46]
- Service providers and advocates could build partnerships with housing providers to help them target more federal rental assistance for supportive housing. State and local program administrators can target vouchers and subsidized units that become available on specific populations to provide supportive housing, but they are not required to, and few currently do so.[47]
- State and federal policymakers could direct more development resources to supportive housing. Especially in certain high-cost, low-vacancy areas and some rural areas where rental assistance alone may be difficult to use, development subsidies are needed to create more supportive housing. The federal Low Income Housing Tax Credit (LIHTC) is the largest source of development funds,[48] and the National Housing Trust Fund (NHTF)[49] will become another important source of development funding beginning this year. The NHTF requires that the housing be targeted on much lower-income households than LIHTC. Coupling project-based Housing Choice Vouchers with LIHTC or other development funds can be especially helpful for building or rehabilitating new supportive housing. The dedicated income that a project-based voucher ensures can help to raise additional funding for a project, possibly increasing the number of units that get built. State agencies that allocate tax credits and trust funds to projects could better target them for supportive housing, based on an assessment of local need. To be most effective in increasing the availability of supportive housing, any federal expansion of development funds should also include an expansion of rental assistance.
Reinvesting Savings
States and localities should reinvest some of the savings that supportive housing produces in systems like corrections and health care to provide more rental assistance. To produce savings sufficient to merit reinvestment, states or localities must target individuals who are the costliest users of these systems. While demonstrating savings and achieving consensus on reinvestment can be significant challenges, states may be best situated to create such initiatives, since a state could aggregate savings from multiple systems. If the savings are large enough, counties, cities, and other entities (see example below) could reinvest savings as well.
California and New York are taking steps, through section 1115 Medicaid waivers, to reinvest savings in supportive housing. California now explicitly offers counties the opportunity to form pilots that allow entities in the county, including health care plans, public hospitals, charitable organizations, and others, to contribute to county-based housing funding pools. Contributions can come from savings achieved in reduced jail, emergency room and homeless shelter utilization by implementing programs such as supportive housing. The pilot can reinvest the funds in these pools to expand affordable housing, which may help further drive down costs if this housing is targeted to costly groups and combined with services.[50] New York is projecting potential state health care savings from supportive housing and using those funds to provide rental assistance and capital grants for supportive housing.[51] Neither model has been fully implemented yet, and accurately tracking the savings is difficult, but they present promising paths forward for this approach.
A number of communities have employed an innovative practice called Pay for Success financing to help build the evidence for creating savings through supportive housing. Pay for Success is a public-private partnership in which private investors provide the necessary up-front funding to initiate a certain program (like supportive housing) with clear goals and are paid back only if the program meets those goals. Some communities have used this model to fund supportive housing to reduce costs in health care or corrections. While few of these initiatives have results yet, and they are not a substitute for additional government investment in supportive housing, Pay for Success is another promising approach to help jumpstart new supportive housing initiatives.
Increasing the Use of Medicaid to Provide Supportive Services
Most federal grant programs that fund supportive services are time-limited and funded at levels too low to meet the need (see appendix for a list of the major federal services programs). Medicaid is available to anyone who qualifies, so it provides a much larger, more predictable source of health and supportive services funding. Some states have increasingly leveraged Medicaid as a source of services funding for supportive housing, but it is still underutilized for this purpose. States can take multiple steps to expand the availability of services for supportive housing through Medicaid. They can:
- Expand Medicaid. Health reform gave states the opportunity to expand their Medicaid programs to cover nearly everyone whose income is at or below 138 percent of the poverty line, which includes most people who need supportive housing. But 19 states have not expanded Medicaid, and in those states, only people with certain disabilities, seniors, or low- income families with children are eligible. Barriers to proving disability status preclude many from Medicaid eligibility, especially homeless people with mental illness or substance use disorders. Expanding Medicaid in the states that have not done so would be an important step toward providing supportive housing for more of those who need it. Without expansion, other policy changes, such as those outlined below, will have a limited impact, since they will reach only a fraction of those who need supportive housing.
- Provide a broader range of Medicaid-funded services and supports, including services to help find and maintain housing. States need to make changes to their Medicaid programs to better provide services for supportive housing. Most health services available through Medicaid to help people stay in their homes are services that states are allowed but not required to offer, and many state Medicaid programs do not cover them. The federal Centers for Medicare and Medicaid Services (CMS) recently described how Medicaid can provide services for supportive housing.[52] Medicaid can provide services such as personal care services in homes, behavioral health care services, intensive case management, and housing-specific supports like help searching for housing and working with landlords, if these services are necessary for someone to maintain their health and keep them out of expensive institutional care. More states should take advantage of the flexibility they have to provide these services.
- Institute a process for supportive housing providers to secure Medicaid reimbursement where appropriate. Most supportive housing providers have not traditionally billed Medicaid for various services that are eligible for Medicaid reimbursement. States and managed care organizations should provide training and outreach to encourage supportive housing providers to bill Medicaid where that is appropriate. This would help ensure that Medicaid-funded supportive housing services are provided mainly by organizations with supportive housing experience.
- Deliver support services in a more coordinated fashion. Medicaid services are not always delivered in a way that fits the supportive housing model. Services are often delivered only within the confines of an office, without coordination among providers. Moreover, providers may not focus on preventing emergency room visits or other unnecessary treatment. States could institute reforms in their health care systems to give hospitals, community health centers, and other providers incentives to provide the mobile, team-based services required for supportive housing, and focus on providing more appropriate care. To achieve reforms, states can apply for waivers to some Medicaid rules and amend their Medicaid state plans.[53]
- Use managed care more effectively. Increasingly, states are relying on managed care organizations (MCOs) to provide and coordinate health benefits for Medicaid beneficiaries. MCOs receive a set payment from the state per enrollee and are required to provide all needed services to their members, based on their contract with the state. In addition to the services they are contractually required to provide, MCOs have some flexibility to provide mobile, flexible services and have helped some states provide supportive housing services. States can require MCOs to provide supportive housing services to those who need them, and MCOs can work with supportive housing providers to make sure their members receive the right level of care.
If more states took these steps, more Medicaid services could be used in place of the services provided through limited grant dollars, freeing up those scarce resources to fill other needs. States that increase Medicaid services for supportive housing should also consider reinvesting some of the potential health care savings to provide additional rental assistance.
Targeting Supportive Housing on Those Who Need It
Many people, even those with disabilities, are able to remain stably housed without supportive housing’s intensive services. To best use available resources, supportive housing providers should ensure they admit only those who cannot succeed with a lower level of care. In addition, a system should be in place to move people who no longer need supportive housing into lower levels of support.
There is currently no single standardized assessment that differentiates between people who need supportive housing and those who do not. Providers often create their own assessments to target supportive housing on people who have been homeless for long periods of time, have multiple disabilities, have failed to remain healthy or stably housed with other treatments, or use health care and corrections frequently.
Yet no measure is perfect, and people will differ significantly in how long they need supportive housing. So supportive housing providers must also have a process to move people to less intensive supports, though they likely will continue to need long-term rental assistance to afford housing in the community. Such a “moving-on” system is relatively simple in supportive housing that links tenant-based rental assistance with community-based service providers. These service providers, some of whom receive Medicaid reimbursement for their services, can serve anyone regardless of where they live and can adjust to provide a lower level of care.
Supportive housing that is provided through project-based rental assistance needs more coordination to allow people to move out while retaining their rental assistance. The building may be configured specifically to provide certain services (like having a clinic or therapist’s office on site), and someone remaining there who no longer needs a high level of support would prevent someone else from receiving it. Housing Choice Vouchers are especially helpful in this situation, since people in units with project-based vouchers are allowed to move out with an available tenant-based voucher.[54] Other forms of project-based assistance do not have this option, but providers can work with their local or state public housing agency to target some tenant-based Housing Choice Vouchers for former supportive housing tenants to create a similar system.
Appendix: Federal Resources for Supportive Housing
| TABLE 1 | ||||
|---|---|---|---|---|
| Federal Rental Assistance | ||||
| Households using rental assistance | Eligibility | Grantees must provide services? | Administering entity | |
| Housing Choice Vouchers | 2,164,000 | Low-income1 | No | State/local public housing agency |
| Public Housing | 1,049,000 | Low-income | No | State/local public housing agency |
| Section 8 project-based | 1,170,000 | Low-income | No | Private owners |
| McKinney-Vento Homeless Assistance Permanent Supportive Housing | 138,000 | Disability, homeless, low-income | Yes | Continuum of Care |
| Elderly (202) | 120,000 | Age >62, low-income | No | Private owners |
| Disabled (811) | 33,000 | Disability, low-income | No | Private owners |
| Housing Opportunities for People with HIV/AIDs | 25,000 | HIV+, low-income | Yes | States and localities |
| USDA rural rental assistance | 273,000 | Low-income | No | Private owners |
| TABLE 2 | |||||
|---|---|---|---|---|---|
| Federal Funding for Supportive Housing Services1 | |||||
| Program | FY2016 budget authority (millions) | Target population | Federal agency | Activities | Administering entity |
| Community Health Centers/Health Care for the Homeless2 | $5,091 | Low-income communities without access to health care | HHS Health Resources and Services Administration (HRSA) | Primary and behavioral health care | Community health centers |
| Ryan White HIV/AIDS Program | $2,323 | People living with HIV/AIDS | HHS HRSA | Primary health care | Municipalities |
| Substance Abuse Prevention and Treatment Block Grant | $1,858 | People with substance use disorders | HHS Substance Abuse and Mental Health Services Administration (SAMHSA) | Substance use and prevention services only | States |
| Social Services Block Grant | $1,669 | Broad, low-income and vulnerable people | HHS Office of Community Services | Multiple, including case management, housing, and substance use services | States |
| Community Services Block Grant | $715 | People and families in poverty | HHS Office of Community Services | Multiple, focus on reducing poverty | States, community action agencies |
| Community Mental Health Services Block Grant | $533 | Adults with serious mental illness and children with serious emotional disorders | HHS SAMHSA | Mental health services only, including in supportive housing | States |
| Promoting Safe and Stable Families | $381 | Families involved in the child welfare system | HHS Administration for Children and Families | Family preservation and reunification | States |
| Supportive Services for Veteran Families3 | $300 | Homeless veterans | Veterans Affairs | Linkage to housing and long-term supports | Local non-profits |
| Homeless Services Grants | $74 | Homeless people with mental illness or substance use disorders | HHS SAMHSA | Mental health and substance use services, especially for supportive housing | States, localities, and non-profits |
| Second Chance Act3 | $68 | People returning from prison or jail | Department of Justice | Linkage to services and supports, including housing and mental health and substance use services | Government agencies and non-profits |
| Projects for Assistance in Transition from Homelessness3 | $65 | Homeless people with serious mental illness | HHS SAMHSA | Linkage to housing and long-term supports | States |
| Homeless Veterans Reintegration Program | $38 | Homeless veterans | Department of Labor | Employment and training | State and local organizations |
| Runaway and Homeless Youth Street Outreach3 | $17 | Homeless youth | HHS ACF | Street outreach, housing search | Local non-profits |
End Notes
[1] We are grateful to The Kresge Foundation and the Melville Charitable Trust for their support of this paper.
[2] There are a number of well-designed experimental and quasi-experimental studies, as well as a large body of case studies for these groups. For reviews, see Carol L.M. Caton, Carol Wilkins, and Jacquelyn Andersen, “People Who Experience Long-Term Homelessness,” chapter 4 in Deborah Dennis, Gretchen Locke, and Jill Khadduri, eds., Toward Understanding Homelessness: The 2007 National Symposium on Homelessness Research, Department of Health and Human Services and U.S. Department of Housing and Urban Development, September 2007, https://aspe.hhs.gov/execsum/toward-understanding-homelessness-2007-national-symposium-homelessness-research; Thomas Byrne et al., “The Relationship between Community Investment in Permanent Supportive Housing and Chronic Homelessness,” Social Service Review, June 2014, Vol. 88, No. 2, pp. 234-263; Debra Rog et al., “Permanent Supportive Housing: Assessing the Evidence,” Psychiatric Services, March 2014, Vol. 65, No. 3, pp. 287-294.
[3] “No Strings Attached: Helping Vulnerable Youth with Non-Time-Limited Supportive Housing” CSH, March 2016, http://www.csh.org/wp-content/uploads/2016/03/CSH_NonTimeLimitedYouthSH_3.25.16.pdf.
[4] Frank R. Lipton et al. “Tenure in Supportive Housing for Homeless Persons with Severe Mental Illness,” Psychiatric Services, April 2000, Vol. 51, No. 4, pp 479-486.; Sam Tsemberis and Ronda Eisenberg, “Pathways to Housing: Supported Housing for Street-Dwelling Homeless Individuals with Psychiatric Disabilities,” Psychiatric Services, April 2000, Vol. 51, No. 4, pp. 487-493.
[5] Robert Rosenheck et al., “Cost-Effectiveness of Supported Housing for Homeless Persons with Mental Illness,” Archives of General Psychiatry, September 2003, Vol. 60, No. 9, pp. 940-951.
[6] Stephen H. Leff et al., “Does One Size Fit All? What We Can and Can’t Learn from a Meta-Analysis of Housing Models for Persons with Mental Illness,” Psychiatric Services, April 2009, Vol. 60, No. 4, pp. 473-482.
[7] Laura S. Sadowski et al., “Effect of a Housing and Case Management Program on Emergency Department Visits and Hospitalizations Among Chronically Ill Homeless Adults,” Journal of the American Medical Association, May 2009, Vol. 301, No. 17, pp. 1771-1778.
[8] Dennis P. Culhane, Stephen Metraux, and Trevor Hadley, “Public Service Reductions Associated with Placement of Homeless Persons with Severe Mental Illness in Supportive Housing,” Housing Policy Debate, 2002, Vol. 13, Issue 1, pp. 107-163.
[9] Metraux and Culhane (2004) found that 45 percent of those leaving jails or prisons with a prior history of homeless shelter use reentered shelters, mostly within the first month of release. People who had contact with the mental health system had more shelter stays and re-incarcerations than those who had not. Similarly, Culhane, Metraux, and Hadley (2002) found that, among people experiencing homelessness entering supportive housing in New York City, 26 percent had stayed in a state run psychiatric hospital in the two years prior to moving into supportive housing. Hopper et al. (1997) conducted in-depth interviews with 36 people experiencing homelessness. They identified a sub-set of these individuals who lived in an “institutional circuit” — they spent some time homeless, but they spent about 40 percent of their time cycling between hospitals, psychiatric institutions, and prisons and jails.
Stephen Metraux and Dennis Culhane, “Homeless Shelter Use and Reincarceration Following Prison Release,” Criminology and Public Policy, 2004, Vol. 3, No. 2, pp. 139-160; Culhane, Metraux, and Hadley, 2002; Kim Hopper et al., “Homelessness, Severe Mental Illness, and the Institutional Circuit,” Psychiatric Services, May 1997, Vol. 48, No. 5, pp. 659-664.
[10] Culhane, Metraux, and Hadley, 2002.
[11] Studies include between 25 and 80 people.
[12] Leyla Gulcur et al., “Housing, Hospitalization, and Cost Outcomes for Homeless Individuals with Psychiatric Disabilities Participating in Continuum of Care and Housing First Programmes,” Journal of Community & Applied Social Psychology, April 2003, Vol. 13, pp. 171-186.
[13] Jocelyn Fontaine et al., “Supportive Housing for Returning Prisoners: Outcomes and Impacts of the Returning Home Ohio Pilot Project,” Urban Institute, August 2012, http://www.urban.org/sites/default/files/alfresco/publication-pdfs/412632-Supportive-Housing-for-Returning-Prisoners-Outcomes-and-Impacts-of-the-Returning-Home-Ohio-Pilot-Project.PDF.
[14] Rosenheck et al., 2003.
[15] Stephen Poulin et al., “Service Use and Costs for Persons Experiencing Chronic Homelessness in Philadelphia: A Population-Based Study,” Psychiatric Services, November 2010, Vol. 61, No. 11, pp. 1093-1098.
[16] High-need participants were identified using screening tools that indicate low ability to function in the community and high mental health needs, and they had to have a history of hospitalization due to mental illness, co-occurring substance use disorder, or a recent arrest or incarceration. Moderate-need participants included everyone who didn’t fit into the high-need category. See http://bmjopen.bmj.com/content/1/2/e000323.full.pdf+html for more information.
[17] Paula Goering et al., “National At Home/Chez Soi Final Report,” Calgary, AB: Mental Health Commission of Canada, 2014, http://www.mentalhealthcommission.ca.
[18] Anirban Basu et al., “Comparative Cost Analysis of Housing and Case Management Program for Chronically Ill Homeless Adults Compared to Usual Care,” Health Services Research, February 2012, Vol. 47, No. 1, Part II, pp. 523-543.
[19] These reductions are reported as annualized averages. The researchers averaged the intervention group’s changes in health care utilization during the 18-month study period and adjusted the utilization to be equivalent to health care use in one year.
[20] David Buchanan et al., “The Health Impact of Supportive Housing for HIV-Positive Homeless Patients: A Randomized Controlled Trial,” American Journal of Public Health, November 2009, Vol. 99, No. S3, pp. 675-680.
[21] The researchers define “intact immunity” as having a CD4 count above 200 and viral load below 100,000.
[22] Sandra K. Schwarz et al., “Impact of Housing on the Survival of Persons with AIDs,” BMC Public Health, July 2009, http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-9-220.
[23] Debra Rog et al., 2014; Martha Burt, Carol Wilkins, and Danna Mauch, “Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Literature Synthesis and Environmental Scan,” Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, January 6, 2011, https://aspe.hhs.gov/pdf-report/medicaid-and-permanent-supportive-housing-chronically-homeless-literature-synthesis-and-environmental-scan.
[24] Sam Tsemberis, Leyla Gulcur, and Maria Nakae, “Housing First, Consumer Choice, and Harm Reduction for Homeless Individuals With a Dual Diagnosis,” American Journal of Public Health, April 2004, Vol. 94, No. 4, pp. 651-656.
[25] An-Lin Cheng et al., “Impact of Supported Housing on Clinical Outcomes Analysis of a Randomized Trial Using Multiple Imputation Technique,” Journal of Nervous and Mental Disease, January 2007, Vol. 195, No. 1, pp. 83-88.
[26] The original analysis of the data found no difference in alcohol or drug use between those with and without supportive housing, but a substantial amount of the data for the non-supportive housing groups was missing. A subsequent analysis that adjusted for the missing data found large reductions in alcohol and drug use.
[27] Martha Burt, Carol Wilkins, and Danna Mauch, 2011.
A study of the Downtown Emergency Services Center’s 1811 Eastlake property found that even people with severe alcohol problems reduced their alcohol use in supportive housing. See Mary E. Larimer et al., “Health Care and Public Service Use and Costs Before and After Provision of Housing for Chronically Homeless Persons with Severe Alcohol Problems,” JAMA, (2009), Vol. 301, No. 13, pp. 1349-1357.
[28] Caton, Wilkins, and Andersen, 2007.
[29] Sune Rubak et al., “Motivational interviewing: a systematic review and meta-analysis,” British Journal of General Practice, April 2005, Vol. 55, No. 513, pp. 305–312, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1463134/.
[30] In 2014, over 7 percent of people in supportive housing for the homeless were 62 or older, and that number will likely grow as the population ages. See “The 2014 Annual Homeless Assessment Report (AHAR) to Congress, Part 2: Estimates of Homelessness in the United States,” U.S. Department of Housing and Urban Development, Office of Community Planning and Development, https://www.hudexchange.info/resource/4828/2014-ahar-part-2-estimates-of-homelessness/.
[31] Nicholas Castle and Neil Resnick, “Service-Enriched Housing: The Staying at Home Program,” Journal of Applied Gerontology, July 2014, pp. 1-21.
[32] Seniors did not differ in demographics or functional status across the intervention and control groups.
[33] Arkadipta Ghosh, Cara Orfield, and Robert Schmitz, “Evaluating PACE: A Review of the Literature,” prepared for the Office of Disability, Aging, and Long-Term Care Policy, and the Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, January 2014, https://aspe.hhs.gov/pdf-report/evaluating-pace-review-literature; Ruth Elkan, et al., “Effectiveness of Home-based Support for Older People: Systematic Review and Metaanalysis,” BMJ, September 2001, Vol. 323, No. 7315, pp. 719-725.
[34] “The Minnesota Supportive Housing and Managed Care Pilot: Evaluation Summary,” prepared for Heart Connection by the National Center on Family Homelessness, March 2009, http://www.air.org/sites/default/files/downloads/report/Evaluation-Minnesota-Supportive-Housing-and-Managed-Care-Pilot-2009.pdf.
[35] Debra J. Rog and John C. Buckner, “Homeless Families with Children,” Chapter 5 in Toward Understanding Homelessness: The 2007 National Symposium on Homelessness Research, eds. Deborah Dennis, Gretchen Locke, and Jill Khadduri, U.S. Department of Health and Human Services and Department of Housing and Urban Development, September 2007, https://aspe.hhs.gov/legacy-page/2007-national-symposium-homelessness-research-homeless-families-and-children-146546.
[36] Daniel Gubits et al., “Family Options Study: Short-Term Impacts of Housing and Services Interventions for Homeless Families,” Office of Policy Development and Research, U.S. Department of Housing and Urban Development, July 2015, https://www.huduser.gov/portal/family_options_study.html.
[37] Anthony L. Loman, “Families Frequently Encountered by Child Protection Services: A Report on Chronic Child Abuse and Neglect,” Institute of Applied Research, February 2006, http://www.iarstl.org/papers/FEfamiliesChronicCAN.pdf.
[38] Rebecca Swann-Jackson, Donna Tapper, and Allison Fields, “Keeping Families Together: An Evaluation of the Implementation and Outcomes of a Pilot Supportive Housing Model for Families Involved in the Child Welfare System,” Metis Associates, November 2010, http://www.csh.org/wp-content/uploads/2011/12/Report_KFTFindingsreport.pdf.
[39] Mary Cunningham et al., “Supportive Housing for High-Need Families in the Child Welfare System,” Urban Institute, November 2014, http://www.urban.org/research/publication/supportive-housing-high-need-families-child-welfare-system.
[40] Over 96,000 people were classified as chronically homeless (a small subset of the total homeless population which usually need supportive housing), including more than 13,000 people in families with children, on one night in January 2015. About 95,000 beds in supportive housing were dedicated to this group that year. People are classified as chronically homeless if they have disabilities and have experienced at least 12 months of homelessness, either continuously or cumulatively over three years.
There are another 224,146 beds in supportive housing for people with disabilities who are homeless but not chronically. Some 488,000 adults spent at least one night in a homeless shelter during 2014 and had a disability, but not all these adults would need supportive housing. In total, 1.488 million people spent at least one night in a shelter in 2014. Likely some small portion of this total also need supportive housing but were not identified as having a disability.
There are at least hundreds of thousands of additional people who live in in nursing homes, psychiatric institutions, jails, and prisons and could move into the community with supportive housing, but the exact number who need supportive housing (as opposed to affordable housing with less intensive services) is unknown. Supportive housing does exist for these groups, but there are no accurate counts of the number of units.
“The 2015 Annual Homeless Assessment Report to Congress, Part 1: Point-in-Time Estimates of Homelessness.” U.S. Department of Housing and Urban Development Office of Community Planning and Development, November 2015, https://www.hudexchange.info/resources/documents/2015-AHAR-Part-1.pdf; “The 2014 Annual Homeless Assessment Report to Congress, Part 2: Estimates of Homelessness in the United States,” U.S. Department of Housing and Urban Development Office of Community Planning and Development, November 2015, https://www.hudexchange.info/onecpd/assets/File/2014-AHAR-Part-2.pdf.
[41] See Part VI of Barbara Sard and Will Fischer, “Chart Book: Federal Housing Spending Is Poorly Matched to Need,” Center on Budget and Policy Priorities, December 18, 2013, https://www.cbpp.org/research/chart-book-federal-housing-spending-is-poorly-matched-to-need.
[42] Policymakers have funded about 80,000 Housing Choice Vouchers for homeless veterans with disabilities, called Veterans Affairs Supportive Housing vouchers (or HUD-VASH), since 2008. Veteran homelessness declined 36 percent between 2010 and 2015.
[43] The three largest rental assistance programs are Housing Choice Vouchers, Public Housing, and Project-Based Rental Assistance (PBRA). Policymakers ceased the expansion of Public Housing and PBRA in the mid-1990s. For more information see the Center’s Policy Basics on Housing Choice Voucher, Public Housing, and Project-Based Rental Assistance programs: https://www.cbpp.org/research/housing/policy-basics-the-housing-choice-voucher-program; https://www.cbpp.org/research/policy-basics-introduction-to-public-housing; and https://www.cbpp.org/research/housing/policy-basics-section-8-project-based-rental-assistance.
[44] Public housing agencies dedicate project-based vouchers to specific units by contract, for an initial term of up to 15 years. For more information see the Center’s Policy Basics: Project-Based Vouchers.
[45] “The 2015 Annual Homeless Assessment Report to Congress, Part 1: Point-in-Time Estimates of Homelessness,” U.S. Department of Housing and Urban Development Office of Community Planning and Development, November 2015, https://www.hudexchange.info/resources/documents/2015-AHAR-Part-1.pdf.
[46] Rachel Bergquist et al., “State Funded Housing Assistance Programs,” Technical Assistance Collaborative, April 2014, http://www.tacinc.org/media/43566/State%20Funded%20Housing%20Assistance%20Report.pdf.
[47] Less than a quarter of PHAs target some of their Public Housing or Housing Choice Vouchers toward homelessness or reduce screening barriers for homeless households. See “Study of PHAs’ Efforts to Serve People Experiencing Homelessness,” U.S. Department of Housing and Urban Development Office of Policy Development and Research, https://www.huduser.gov/portal/publications/pdf/pha_homelessness.pdf.
[48] Investors fund part of the cost of supportive housing development by purchasing credits that states allocate to particular developments; in exchange, the credits reduce their federal tax liability.
[49] See the National Low Income Housing Coalition’s “National Housing Trust Fund Resources” page, http://nlihc.org/issues/nhtf/resources, for more information.
[50] This was done using a Medicaid 1115 waiver, which can be used for demonstration projects meant to test new service delivery and payment models. These waivers must be budget neutral for the federal government and include an evaluation component. States can use these waivers to test adding new benefits to their Medicaid program and directing those services to a particular subset of their Medicaid-eligible beneficiaries. California’s new waiver was approved in December 2015.
[51] See the Supportive Housing Network of New York’s “Medicaid Redesign” page, http://shnny.org/budget-policy/state/medicaid-redesign/, for more information on New York’s supportive housing plan.
[52] Vikki Wachino, “Coverage of Housing-Related Activities and Services for Individuals with Disabilities,” Center for Medicaid & CHIP Services, June 26, 2015, https://www.medicaid.gov/federal-policy-guidance/downloads/cib-06-26-2015.pdf.
[53] See CSH’s “A Quick Guide to Improving Medicaid Coverage for Supportive Housing Services” for detailed information about various Medicaid waivers and state plan options, http://www.csh.org/wp-content/uploads/2015/05/A-Quick-Guide-To-Improving-Medicaid-Coverage-For-Supportive-Housing-Services1.pdf.
[54] For more information see the Center’s Policy Basics: Project-Based Vouchers.
More from the Authors


Areas of Expertise

Areas of Expertise
