WIC Works: Addressing the Nutrition and Health Needs of Low-Income Families for More Than Four Decades
Extensive research has found the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) to be a cost-effective investment that improves the nutrition and health of low-income families — leading to healthier infants, more nutritious diets and better health care for children, and subsequently to higher academic achievement for students. As a result of the research documenting WIC’s effectiveness, Administrations and Congresses of both parties have provided sufficient funding since 1997 to ensure that WIC can serve all eligible low-income pregnant women, infants, and young children who apply for it.
What Works to Reduce Poverty
As part of Policy Futures, we examine “what works” when it comes to federal and state policies and programs to reduce poverty and promote opportunity for low-income Americans. We synthesize and amplify the work of poverty researchers around the country on program effectiveness. This effort is designed to inform discussions about new investments in anti-poverty programs as well as reforms of, and funding levels for, existing programs.
WIC provides nutritious foods, nutrition education, breastfeeding support, and referrals to health care and social services for millions of low-income families, and it plays a crucial role in improving lifetime health for women, their infants, and young children. Part of the nation’s nutrition safety net for over 45 years, WIC now serves over 6 million pregnant and post-partum women, infants, and children through their fifth birthday. For a family to participate, it must have gross income of no more than 185 percent of the federal poverty level (now $40,182 for a family of three) and be at nutritional risk. To simplify program administration, an applicant who already receives SNAP (formerly food stamps), Medicaid, or Temporary Assistance for Needy Families cash assistance is automatically considered income-eligible.[2]
Over more than four decades, researchers have investigated WIC’s effects on key measures of child health such as birth weight, infant mortality, diet quality and nutrient intake, initiation and duration of breastfeeding, cognitive development and learning, immunization, use of health services, and childhood anemia. Two comprehensive reviews of the research literature catalogued the findings on WIC’s effectiveness through 2010.[3] This paper builds on those reviews, extending the evidence from earlier studies with more recent research. Taken as a whole, the evidence demonstrates WIC’s effectiveness.
- Women who participate in WIC give birth to healthier babies who are more likely to survive infancy.
- WIC supports more nutritious diets and better infant feeding practices. WIC participants buy and eat more fruits, vegetables, whole grains, and low-fat dairy products, following the introduction of improved WIC food packages more closely aligned to current dietary guidance.
- Low-income children participating in WIC are just as likely to be immunized as more affluent children, and are more likely to receive preventive medical care than other low-income children.
- Children whose mothers participated in WIC while pregnant scored higher on assessments of mental development at age 2 than similar children whose mothers did not participate, and they later performed better on reading assessments while in school.
- Improvements made to the WIC food packages since 2009 have contributed to healthier food environments in low-income neighborhoods, enhancing access to fruits, vegetables, and whole grains for all consumers regardless of whether they participate in WIC.
Why the Early Years Are So Important
It has long been recognized that children living in poverty lag behind other children on a wide range of indicators of physical, mental, academic, and economic well-being.[4] They are more likely to have health, behavioral, learning, and emotional problems. This is especially true of children whose families experience deep poverty, those who are poor during early childhood, and those who are poor for a long time. Children living in poverty are also more likely to be food insecure, and food insecurity in households with children is associated with inadequate intake of several important nutrients, deficits in cognitive development, behavioral problems, and poor health.[5] Recent research indicates that significant disparities in early childhood development — including physical health and well-being, social competence, emotional maturity, language and cognitive development, and general knowledge and communication skills — are associated with neighborhood income, race, and ethnicity by the time children reach kindergarten.[6]
Mounting evidence suggests that the consequences of adversity during early childhood can extend well beyond childhood and affect physical, mental, and economic well-being throughout life.[7] Researchers at Harvard University’s Center on the Developing Child, for example, write that:
Toxic stress experienced early in life and common precipitants of toxic stress — such as poverty, abuse or neglect, parental substance abuse or mental illness, and exposure to violence — can have a cumulative toll on an individual’s physical and mental health. The more adverse experiences in childhood, the greater the likelihood of developmental delays and other problems.[8]
Poverty in early childhood may be particularly harmful:
Not only does the astonishingly rapid development of young children’s brains leave them sensitive (and vulnerable) to environmental conditions, but the family context (as opposed to schools or peers) dominates children’s everyday lives.[9]
Urban Institute researchers have shown that children who are born into poor families are more likely to drop out of high school, have teen premarital births, have inconsistent employment records, and be poor as adults than children not born poor.[10] Very young children living in food-insecure families are more likely to have low academic scores and to exhibit problem behaviors when they enter kindergarten.[11] Consistent with these findings, increases in family income have been linked to increased school achievement in middle childhood and to greater educational attainment in adolescence and early adulthood.[12] Research on the causal impact of childhood poverty — apart from other disadvantages often associated with poverty that may be detrimental to children, such as low levels of parental education or living with a single parent — reveals that family income early in childhood appears to matter for a range of employment outcomes in adulthood, including earnings and work hours.[13]
Sound investments that reduce early childhood adversity can strengthen the foundations of physical and mental health, with lifelong consequences for educational achievement, economic productivity, health, and longevity.[14] According to the American Academy of Pediatrics:
When developing biological systems are strengthened by positive early experiences, children are more likely to thrive and grow up to be healthy, contributing adults. Sound health in early childhood provides a foundation for the construction of sturdy brain architecture and the achievement of a broad range of skills and learning capacities.[15]
Nutrition influences health at every stage of life.[16] Good nutrition during pregnancy is especially important to support fetal development and protect mothers from pregnancy-related risks of gestational diabetes, excessive weight gain, hypertension, and iron deficiency anemia. Good nutrition in early childhood can promote development and foster healthy behaviors that may carry over into adulthood.
Low-income women and their children may be especially susceptible to the risks of poor nutrition in the early stages of life. Lower socioeconomic status is associated with a wide range of early-life predictors of obesity.[17] And researchers at the University at Buffalo School of Medicine and Biomedical Sciences found substantial differences in the solid foods fed to babies from different socioeconomic classes. Babies of less educated mothers and poorer households were more likely to be fed diets high in sugar and fat, while diets that more closely followed infant feeding guidelines were linked to higher education and higher income.[18] These disparities are important because of evidence that links early postnatal nutrition to long-term health outcomes.[19]
WIC aims to improve the health and nutritional well-being of low-income women and their young children by intervening at critical times of growth and development. Thus, WIC has the potential to improve the life chances of millions of infants and children.
Impacts on Pregnancy and Birth Outcomes
Numerous studies have shown that women who participate in WIC give birth to healthier babies who are more likely to survive infancy. Seminal USDA research early in WIC’s history found that prenatal WIC participation resulted in longer pregnancies, fewer premature births, lower incidence of moderately low and very low birth-weight infants, and fewer infant deaths.[20] While much has changed since those early years, the evidence remains strong that WIC helps improve birth outcomes. Study after study has shown that participation in WIC during pregnancy is associated with longer gestations, higher birth weights, and generally healthier infants, and that the effects tend to be largest for children born to the most disadvantaged mothers.
WIC helps mothers give birth to healthier infants. Maternal and child health experts carefully monitor the birth weight and gestational age of newborns because they are important indicators of an infant’s health and likely survival. Babies born early or with low birth weight (less than 2,500 grams, or about 5.5 pounds) are at higher risk of early death. Low birth-weight babies who survive are more likely to experience cognitive and developmental delays and struggle with disabilities during their childhood and adolescence; they also face higher risks of chronic disease as adults.
WIC supports healthier pregnancies and births by providing the nutritious foods pregnant women and their babies need, referring mothers for essential medical care, and encouraging them to adopt healthy behaviors (such as not smoking during pregnancy).
The available research strongly suggests that women who participate in WIC give birth to healthier infants than eligible non-participants. A review of more than three dozen studies published between 1979 and 2004 concluded that WIC increased average birth weight, reduced the incidence of low birth weight, and improved several other key birth outcomes.[21] A subsequent review of the next generation of studies published through 2010 echoed this conclusion, noting consistent findings that WIC increased average birth weight and reduced the incidence of low and very low birth weight.[22]
More recently, an analysis of a large sample of California births found improvements in a number of maternal and infant health outcomes following the introduction of revised WIC food packages in 2009 (described below), including maternal preeclampsia and weight gain, gestational age at birth, and appropriate birth weight for gestational age. Researchers found, for example, a 17 percent reduction in preeclampsia and an 8 percent reduction in the number of women who gained more weight than recommended.[23] Limited evidence also suggests that participation in WIC may reduce disparities in infant birth weight among more vulnerable women, including the very young, Black women, and those who enter prenatal care relatively late or not at all.[24]
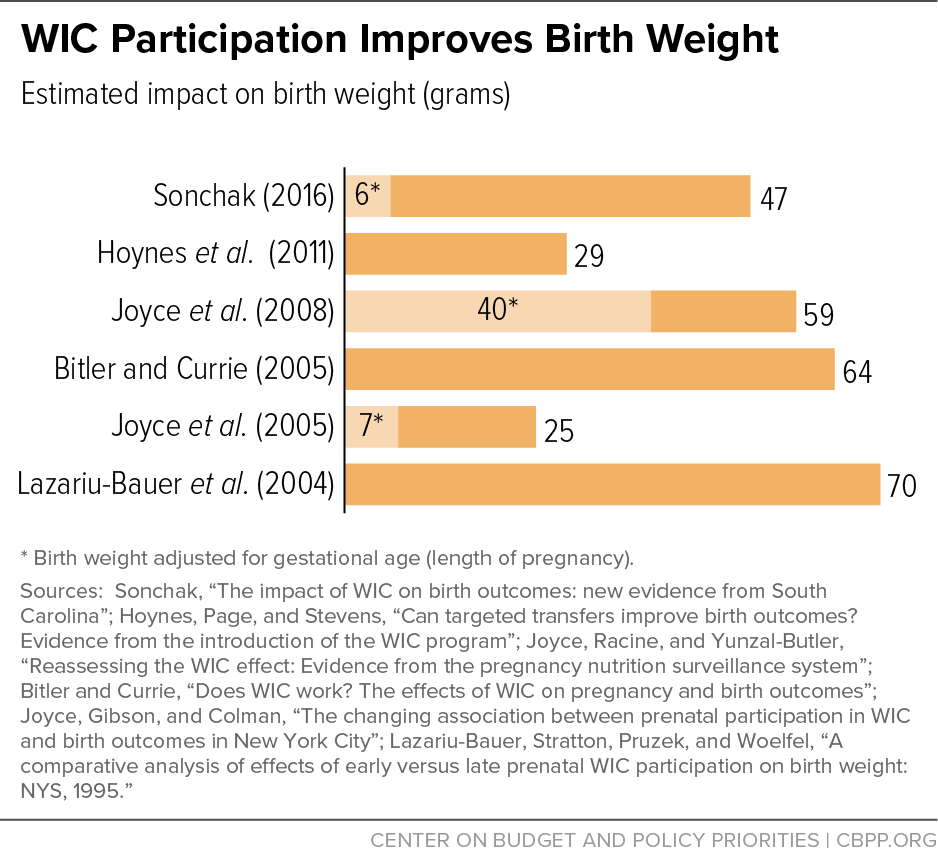
There has been less consensus on the size of WIC’s positive impact. Research in the last 15 years[25] has generally shown that WIC participation is associated with increases in birth weights ranging from about 25 to 70 grams.[26] (See Figure 1.) One influential study estimated that WIC reduced the probability of low birth weight by about 30 percent and the probability of very low birth weight (less than 1,500 grams or 3.3 pounds) by about half.[27] Few of these studies, however, account for the fact that women whose pregnancies last longer have more opportunity to enroll in WIC (see discussion of gestational age bias in the Appendix), so the positive outcomes seemingly associated with WIC participation may reflect the longer pregnancy.
Studies that adjust for gestational age at birth often still find that WIC makes a positive, but more modest, difference. Two studies, for example, report an 11 percent reduction in the incidence of small-for-gestational-age births; a third found infants participating in WIC to be about 6 percent less likely to be low birth weight and 5 percent less likely to be small for gestational age; and another found that Black mothers who participate in WIC are 5 percent less likely to deliver a low birth-weight infant and their infants are 5 percent less likely to be small for gestational age. [28]
It is likely, however, that correcting for gestational age at birth may understate WIC’s positive impact on birth outcomes because it effectively eliminates any positive effect WIC has on extending the duration of healthy pregnancies. Participation in WIC could help extend healthy pregnancies, for example, by better connecting mothers to prenatal health care. Two relatively recent studies take different approaches to address this issue.
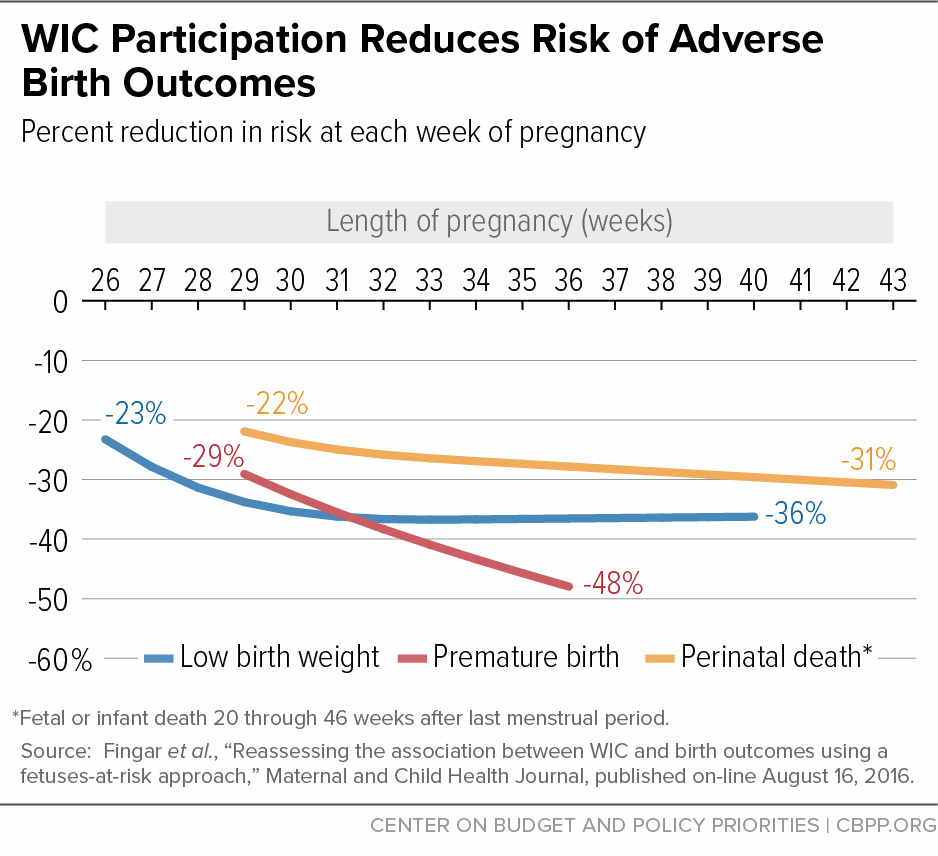
One study used linked birth/death certificate and WIC records in California to compare women eligible for WIC in each week of gestation. This approach addresses gestational age bias by comparing birth outcomes among women whose pregnancies reach the same length and who have the same opportunity to use WIC. This study suggests that participation in WIC is associated with large reductions in the risk of adverse birth outcomes beginning about the 29th week of pregnancy: the risk of premature birth was reduced by 29 to 48 percent, the risk of low birth weight by 23 to 36 percent, and the risk of perinatal death by 22 to 31 percent.[29] (See Figure 2.) The other study, which used a different method to assess the association between WIC participation and gestational age, found that the risk of a preterm birth was reduced by as much as 9 percent for women in Oklahoma and as much as 7 percent in Missouri who began participating in WIC at the beginning of their pregnancy. [30]
Prenatal WIC participation lowers the risk of infant mortality.[31] Infant mortality — death in the first year of life after a live birth — takes a serious toll on the health and well-being of many families and is a key indicator of the health and well-being of communities and the nation. About 22,000 infants die each year, according to the most recent information from the Centers for Disease Control and Prevention (CDC); infant mortality rates are more than twice as high among Black mothers as white mothers. Many factors contribute to infant mortality, including the quality of health care and maternal nutrition.
WIC reduces the risk of infant mortality by connecting expectant mothers to essential prenatal health care, promoting healthy eating through nutrition assessments and counseling, and providing healthy foods tailored to the specific needs of pregnant women and their babies.
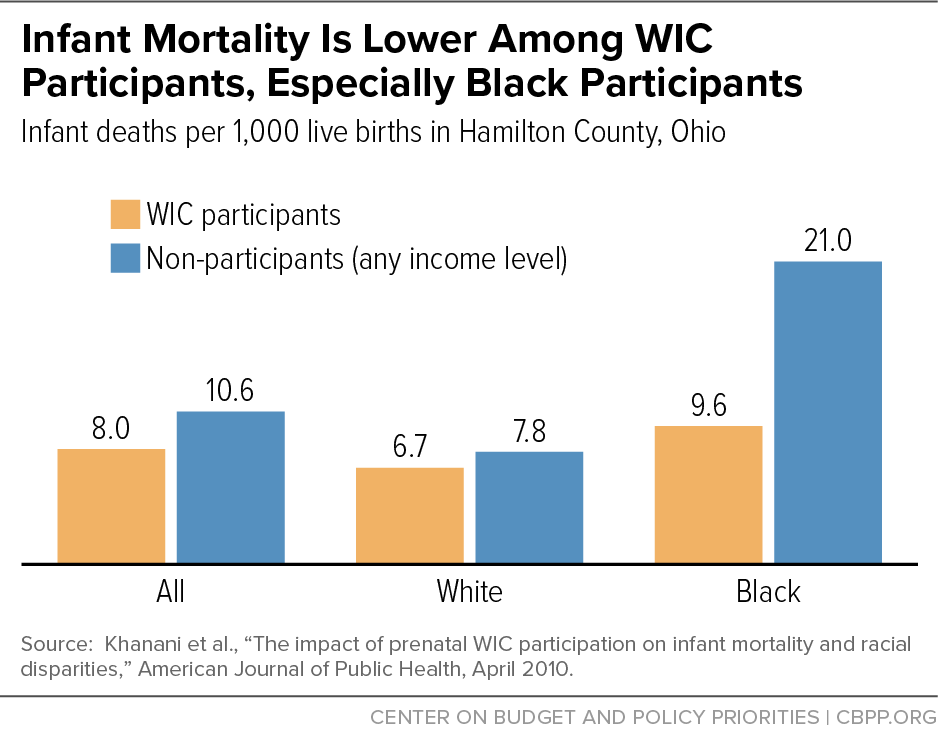
Several early studies suggested that prenatal WIC participation was associated with reductions in infant mortality.[32] Although researchers have paid less attention to this issue since then, a recent study suggests that the risk of infant mortality is lower for babies of mothers who participate in WIC during pregnancy. The infant mortality rate was 5.2 deaths per 1,000 live births among those who had received WIC benefits, compared to 8.2 deaths among those who did not — a 36.6 percent reduction.[33] In addition, researchers in Ohio found a lower infant mortality rate among WIC participants (8.0 infant deaths per 1,000 live births) than non-WIC participants (10.6). (See Figure 3.) The difference was especially striking for Black individuals, with a rate of 9.6 among WIC participants compared to 21.0 among non-WIC participants, significantly reducing the racial disparity between Black and white mothers.[34] A similar examination of infant mortality rates in Kansas found a comparable difference among Black individuals (9.8 among WIC participants compared to 17.7 among non-participants). WIC participation, however, was associated with a slightly higher infant mortality rate among white mothers.[35]
Impacts on Nutrition
WIC supports healthier diets, promotes breastfeeding and better infant feeding practices, and may improve food security among children. Since the introduction of improved food packages better aligned with current dietary guidance, WIC participants are purchasing and consuming more fruits, vegetables, whole grains, and low-fat dairy.
Adequate nutrition during infancy and early childhood is essential to the growth, health, and development of children to their full potential. Moreover, it is important to establish healthful eating behaviors early in life. CDC research teams have linked detailed data on infants’ feeding practices to information on their diet, health, and development six years later to show the importance of early nutrition for long-term health outcomes. Infants who are breastfed longer and introduced to foods or beverages other than breast milk later, for example, tend to have lower rates of ear, throat, and sinus infections by age 6; infants who consume sugar-sweetened beverages are twice as likely to consume them and to be obese at age 6; and infants who consume fruits and vegetables infrequently are more likely to be infrequent consumers at age 6.[36]
WIC provides supplemental foods designed to meet the special nutritional needs of low-income women, infants, and their young children. In December 2007, USDA updated the rules governing WIC foods based on recommendations from the Institute of Medicine to align them more closely with the nutrition science and guidance, including the 2005 Dietary Guidelines for Americans and the American Academy of Pediatrics’ infant feeding practice guidelines. The changes were designed to promote sound nutrition and healthy weight by providing vouchers for fruits and vegetables; adding whole grain and soy products; reducing milk, cheese, and juice allowances; restricting the fat content of milk; reducing saturated fat, cholesterol, and sugar; and giving state agencies more flexibility to accommodate the food preferences of specific cultural groups.[37] All states were required to implement the new food packages by October 2009. In January 2017, the Institute of Medicine (now called the National Academies of Sciences, Engineering, and Medicine) completed a new review and made recommendations to align the food packages with the more recent 2015 Dietary Guidelines, increase flexibility to better support breastfeeding, enhance options to meet cultural needs, and reduce burdens on WIC agencies and vendors.[38]
WIC supports more nutritious diets. Nutrition in infancy and early childhood is critical for optimal growth and development. Food preferences and dietary patterns established during early childhood can lay the foundation for healthy eating habits later in life. Moreover, establishing healthful eating habits early in life can help prevent the onset of diet-related disease.
WIC improves the quality of participants’ diets by providing healthy foods tailored to meet the nutrient needs of mothers and their children during pregnancy, breastfeeding, infancy, and childhood. Participants can use WIC vouchers only for specific healthy foods, such as whole grains, dairy, fish, peanut butter, beans, and fruits and vegetables. In addition, WIC makes nutrition education available to parents and caretakers. Mothers — individually or in groups — meet with a nutritionist, registered dietitian, or trained paraprofessional to learn about the important relationships among nutrition, physical activity, and health. They also discuss issues such as healthy eating during and after pregnancy, developing healthy eating habits in children, reading food labels when shopping, and cooking healthy meals.
There is strong evidence that the introduction of WIC increased infants’ and children’s intakes of some essential vitamins and minerals, especially iron. While vitamin and mineral intake has improved for most children since those early years, research suggests that WIC participation increases the iron density of preschoolers’ diets, reduces the intake of fat as a percentage of food energy, increases the intake of carbohydrates as a percentage of food energy, and reduces consumption of added sugars.[39]
More recently, researchers have focused on the overall diet of infants and toddlers, moving beyond single foods or nutrients. Initial results suggests that infant feeding practices among WIC participants are near optimal in some respects (such as appropriate exposure to iron-rich cereals and limited exposure to energy-dense, low-nutrient food) but have room for improvement in other respects (such as the duration of breastfeeding and frequency of consumption of fruits and vegetables). Similarly, the average Healthy Eating Index (HEI) score of children participating in WIC at ages 13 months and 24 months (64 out of 100), while higher than the U.S. average (59 out of 100), indicates that the average diets of these toddlers do not yet fully conform to dietary recommendations.[40]
Recent research suggests that how long children participate in WIC is significantly associated with the quality of their diets. Children who participated in WIC during most of their first two years of life had better quality diets than children who, despite remaining eligible for benefits, stopped receiving WIC benefits before their first birthday. In addition, research has found that children who received WIC benefits at 24 months consumed more of their daily calories from nutritious WIC-eligible foods than children who did not receive WIC benefits.[41]
The most recent USDA-sponsored research reinforces that consistent participation in WIC through early childhood is associated with better diet quality. Children who participate in WIC through their fourth year have better diet quality as measured by HEI scores than children who leave WIC after their first year. Because 92 percent of mothers participating in WIC during their child’s fourth year value both WIC’s nutrition education and its supplemental foods, these program benefits might contribute to higher diet quality scores among continuous participants.[42]
Other researchers have looked at the type and nutritional quality of foods purchased by WIC participants. One study concludes that participation in WIC is associated with about a 5 percent improvement in nutritional quality of food purchases.[43]Another finds evidence that changes in the food purchases of WIC participants persist even after they leave the program. Specifically, while in the program, participants increase the amount of cereal purchased and shift some of their purchases toward WIC-approved products with less sugar and more whole grains. More importantly, once they leave the program, many continue to purchase the healthier cereals included in the WIC food package. On average, these researchers found that the cereals purchased by WIC participants contained 5.9 percent less sugar and 4.4 percent more fiber. While the improvements in sugar and fiber content of purchased cereals were smaller after leaving WIC, the analysis suggests that program participation may be a potential means to shift food purchases towards healthier choices.[44]
Introduction of the revised food packages enhanced WIC’s impact on healthy diets. Researchers have examined the impact of the food package changes on the food purchases and consumption choices of different groups of participants, in a variety of locales, using a range of research methods. The results are generally consistent: WIC participants receiving the revised food packages purchase and consume more fruits, vegetables, whole grains, and low-fat dairy.[45]
Among all WIC participants, for example, multiple national and state studies suggest a positive relation between the food package revisions and fruit and vegetable purchases or consumption, although the results among smaller local studies are less consistent.[46]
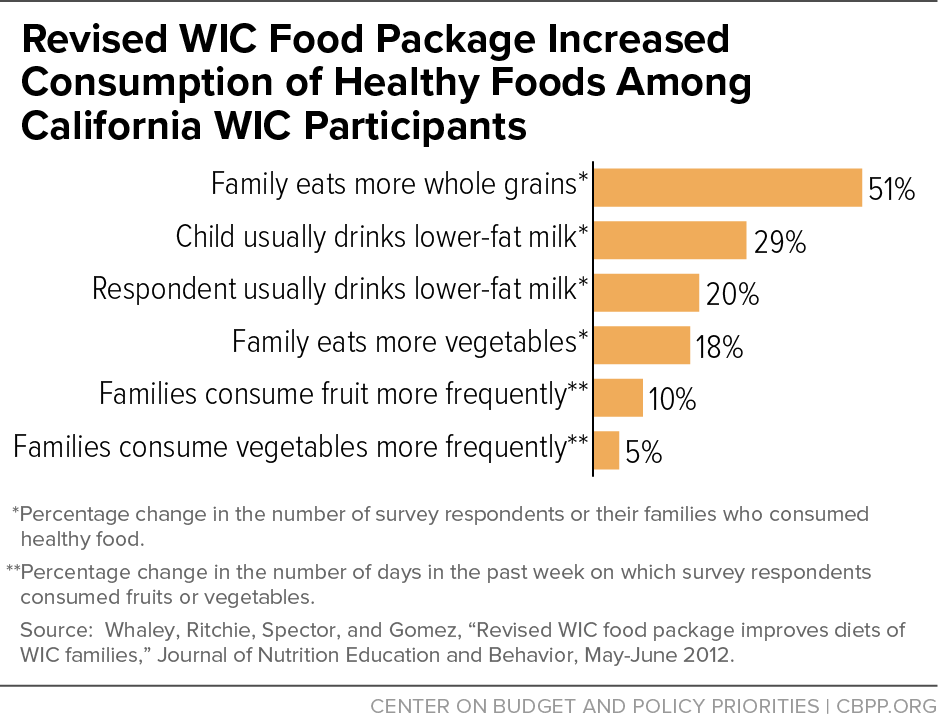
- Surveys of WIC participants in California before and after implementation revealed increases in the consumption of fruit, vegetables, whole grains, and lower-fat milk. Consumption of whole-grain foods increased more than 50 percent; the percentage of caregivers and children who usually consumed lower-fat milk increased by 20 to 30 percent; nearly 20 percent of WIC families ate more vegetables; and the frequency of fruit and vegetable consumption increased by 5 to 10 percent.[47] (See Figure 4.)
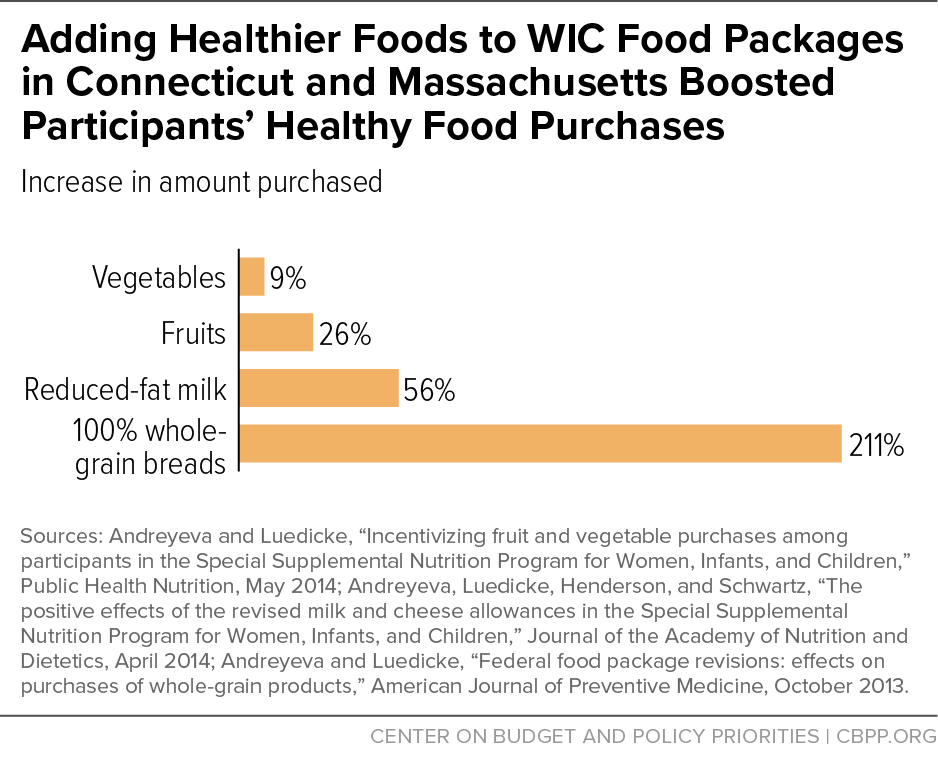
- Scanner data from a New England supermarket chain revealed that WIC participants purchased more vegetables (up 9 percent), fruits (up 26 percent), reduced-fat milk (up 56 percent), and 100-percent whole grain bread (up 211 percent) after implementation of the revised food packages.[48] (See Figure 5.)
Among children receiving WIC, the revised food packages have been associated with improved healthfulness of household food purchases and better dietary quality, as well as reduced risk of obesity.
- Analyses of more than 3.5 million WIC records in New York before and after implementation showed rapid and consistent increases in daily fruit, vegetable, whole grain, and low- and non-fat milk consumption among young children.[49]
- An analysis of packaged food purchases from stores using scanners or smartphone applications found that households participating in WIC made larger reductions in purchases of refined grains and higher-fat milks than low-income non-participants over the five years following introduction of the revised food packages.[50]
- Researchers in Georgia report that Black children participating in WIC significantly increased their intake of low-fat milk after the food package changes. The percentage of children consuming low-fat milk increased from 41 percent before the change to 79 percent four weeks after the change.[51]
- Six months after the WIC food package revisions were implemented, researchers observing the behaviors of Black and Hispanic children and their mothers in 12 WIC clinics in Chicago found a significant decrease in whole-milk consumption, a significant increase in lower-fat milk consumption for all except Black mothers, an increase in fruit consumption among Hispanic mothers, and an increase in the availability of whole grains in the household.[52] A follow-up study after 18 months found continued improvements in intakes of total fat, saturated fat, fiber, and overall dietary quality among Hispanic children. In addition, the prevalence of reduced-fat milk intake significantly increased for Black and Hispanic children, and the prevalence of whole-milk intake significantly decreased for all groups.[53]
- Researchers in Texas report that the probability of consuming whole milk among WIC participants decreased by 45 percent and the probability of consuming reduced-fat milk increased by 33 percent shortly after implementation of the revised food package. In a separate study, they also found increases in lower-fat milk, fruit, vegetable, and whole-grain intake among Native American children.[54]
- Average scores for young, low-income children on the Healthy Eating Index increased more than twice as much (11 percent) among WIC participants as among non- participants (5 percent) between 2003-2008 (before implementation) and 2011-2012 (after implementation).[55]
- Los Angeles County children who participated in WIC continuously from birth to age 4 after introduction of the new food packages had healthier growth trajectories and a 10 to 12 percent lower risk of obesity at age 4 than children who participated continuously before 2009, with the old food packages.[56] Subsequent studies from the same research team concluded that an increase in the amount of breastfeeding and changes in the food packages for children were each partially responsible for the positive effect of the new food packages on obesity.[57]
- The prevalence of obesity across states among 2- to 4-year-old WIC participants — after controlling for sociodemographic characteristics and other obesity risk factors —was increasing before introduction of the revised food packages, but this trend reversed after 2009.[58]
Fewer studies have looked specifically at the impact of the changes to WIC packages for pregnant and post-partum women. Researchers found some moderate improvements in several measures of dietary quality and nutrient intake during pregnancy among women in Memphis and surrounding Shelby County, although these did not persist more than a month after delivery. Another study using national survey data found no evidence of significant improvements in dietary quality among mothers receiving WIC, but the sample of WIC mothers after implementation of the revised food packages may have been too small (just 81 mothers) to detect a meaningful difference.[59]
WIC promotes and supports breastfeeding. Breastfeeding is a beneficial source of nutrition that provides the healthiest start for an infant. The American Academy of Pediatrics recommends that new mothers breastfeed exclusively for about the first six months of a baby’s life and continue for as long as mutually desired by mother and baby.[60] In addition to its nutritional benefits, breastfeeding protects against a number of illnesses and allergies, and is associated with reductions in Sudden Infant Death Syndrome and obesity. It also promotes a unique and emotional connection between mother and baby.[61]
WIC promotes breastfeeding as the optimal infant feeding choice and supports mothers along the way. WIC offers new mothers breastfeeding counseling, peer support, and enhanced benefits (while also providing safe and appropriate food for formula-fed infants). Mothers who choose to breastfeed receive counseling, educational materials, and follow-up support from other mothers with personal experience. Breastfeeding mothers also retain their eligibility for WIC benefits longer. Mothers who exclusively breastfeed receive a food package that is both larger and more varied than the packages provided to mothers who use infant formula.
In general, despite WIC’s strong policy and operational emphasis on promoting breastfeeding, mothers participating in WIC have been less likely than non-participating mothers to breastfeed their infants.[62] Whether this is because providing free infant formula creates an incentive for formula feeding or because mothers who are less likely to breastfeed are also more likely to participate in WIC remains unclear. It is clear, however, that women who are Black, less educated, lower income, or younger are less likely to breastfeed than other women and more likely to participate in WIC. Breastfeeding attitudes and intentions may also matter: women who are still breastfeeding at the time they bring their infants to the WIC clinic for the first time are substantially more likely to have had stronger prenatal intentions, more positive attitudes, and better perceived social supports than mothers who stopped breastfeeding.[63]
The importance of controlling for such differences in the characteristics of mothers who choose to participate in WIC is illustrated in a recent study of a decade of births among women on Medicaid in South Carolina. This research introduced controls for the potential bias caused by self-selection into the program and found that participation in WIC during pregnancy is associated with an overall increase in breastfeeding initiation, driven largely by a nearly 7 percent increase among Black women.[64]
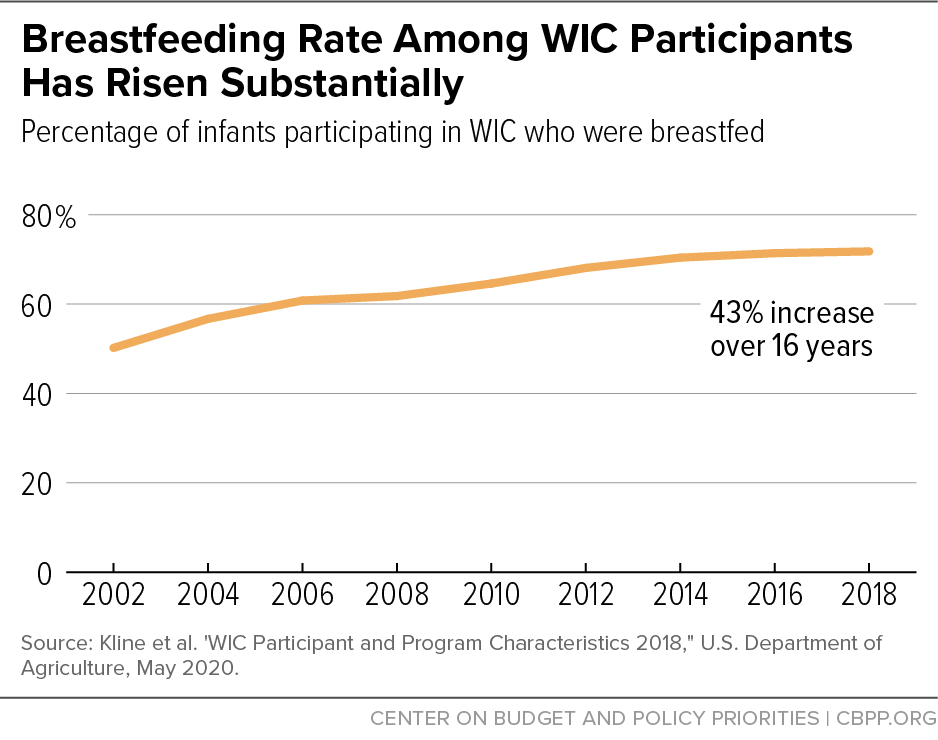
There are indications that the difference between breastfeeding rates among all women and WIC participants has narrowed. Between 2002 and 2017, the percentage of all children who were breastfed increased from 71.4 percent to 84.1 percent.[65] Over roughly the same period (2002 to 2018), the percentage of infants participating in WIC who were breastfed increased from 50.2 percent to 71.8 percent.[66] (See Figure 6.) Thus, while mothers participating in WIC are less likely than others to begin breastfeeding, the gap is substantially smaller than it was.
Recent evidence also suggests that breastfeeding may encourage continued participation in WIC as children grow older. Many families drop out of WIC around the time that children reach their first birthday — at which time eligibility must be recertified and the food package changes from one appropriate for an infant to one for a young child — even though they remain eligible.[67] USDA’s Economic Research Service reports that 23 percent of families participating in WIC during the first year of their infant’s life leave the program around their first birthday.[68] Among predominately Hispanic infants in Southern California, however, those who were fully breastfed during the last half of infancy were three times as likely, and partially breastfed infants were twice as likely, to be recertified as children who were fully formula-fed as infants.[69] And an analysis of national survey data show that infants who were fully breastfed for at least six months are nearly three times as likely to continue on WIC through 2 years of age than infants who were not breastfed.[70]
In response to recommendations from the Institute of Medicine, USDA strengthened the incentives and support for breastfeeding when the new food packages were implemented in 2009. To encourage mothers to begin breastfeeding, WIC no longer routinely provides formula for the first month after birth. To encourage greater duration and intensity of breastfeeding, WIC provides only a limited amount of formula in subsequent months to partially breastfeeding infants. Mothers who require more formula now receive the full-formula food package, even if they are still partially breastfeeding. The full-formula package provides less food for the mother than the partially breastfeeding and fully breastfeeding packages, and the maternal benefits end when the infant is six months old (for the partially or fully breastfeeding packages, they last throughout the infant’s first year).
Even as the Institute of Medicine recommended these changes, there was concern that they might have unintended negative consequences on program participation and breastfeeding practices.[71] Fortunately, USDA’s subsequent evaluation of breastfeeding practices during the first month of infant life found no evidence of adverse impacts.[72]
Moreover, some early evidence suggested that the new policies may encourage breastfeeding, as intended. An expert panel assembled by the Institute of Medicine reviewed the available evidence in 2016 and concluded that “[c]ollectively, the studies suggest that the enhanced food packages, together with improved support for breastfeeding in anticipation of the new packages, may have had a small effect on improving breastfeeding outcomes.”[73] For example, an analysis of WIC administrative records for more than 180,000 infants in Los Angeles found that issuance rates of the fully breastfeeding package at enrollment increased by 86 percent, while issuance rates of packages that included infant formula decreased significantly.[74] In a sample of predominately Latina women in Los Angeles, the prevalence of breastfeeding initiation increased after the implementation of the new food package, and the prevalence of exclusive breastfeeding at three and six months roughly doubled.[75] Finally, a small study in central Texas found small increases in the prevalence of breastfeeding initiation and in breastfeeding duration among WIC infants.[76]
Since then additional research has emerged. An analysis of data collected from participants in roughly 40 states shows that, on average, breastfeeding initiation increased slightly after implementation of the revisions and participants were more likely to receive fully breastfeeding food packages rather than partial breastfeeding packages; there was no significant change in the use of the full-formula package.[77] Another study suggests that the food package revisions may have eliminated the often observed difference in breastfeeding initiation rates between WIC participants and eligible non-participants.[78] The evidence on the relationship between the new food packages and breastfeeding is not yet conclusive, however.[79]
There is also some evidence that early participation in WIC may improve breastfeeding rates. Women who enter WIC in the first trimester of their pregnancy are more likely to begin breastfeeding and continue breastfeeding longer than women who enter in their third trimester.[80] Among mothers with more than one child, for example, early participation in WIC increased the chances of breastfeeding at three months by 15 percent, at six months by 25 percent, and at 12 months by 33 percent.[81]
WIC supports better infant feeding practices. The American Academy of Pediatrics recommends that parents introduce solid foods into their baby’s diet around six months and delay the introduction of cow’s milk until a child’s first birthday. Babies who start eating solid food too early are more likely to be overweight or obese later in life. Cow’s milk is not only difficult for infants to digest but fails to provide all of the fat, calories, and nutrients (especially iron) that babies need to grow well and be healthy.
WIC supports healthy infant feeding by excluding all cow’s milk from infant food packages, introducing infant cereal, fruits, and vegetables at six months, and, for fully breastfed babies, introducing infant meats at six months. The inclusion of infant formula in food packages for those mothers who are unable or choose not to breastfeed ensures that all infants have a safe and appropriate source of good nutrition.
Data from a national survey of infant feeding practices show that the early introduction of solid foods is no longer a major issue among WIC participants. Few mothers participating in WIC (20 percent) introduce cereals, fruits, vegetables, or meat before four months, compared to at least 60 percent 20 years ago. In addition, cow’s milk is introduced to most infants near their first birthday, consistent with current guidance: at eight months of age, only 10 percent of infants have consumed cow’s milk, and by 11 months, 37 percent have. Results from a more recent national survey affirm the conclusion that the overwhelming majority of WIC and other infants do not consume complementary foods before four months.[82]
WIC may improve food security. Food security — access to a safe and secure source of enough food to sustain an active, healthy life — is important for children to develop normally and grow up healthy. Food insecurity among children is associated with many adverse consequences for cognitive development as well as for school readiness, academic performance, and educational attainment; physical, mental, and social health; and behavior. Recent research shows that even marginal food security is associated with poor health and developmental outcomes.[83]
WIC could improve food insecurity and reduce hunger as part of the national nutrition safety net, though these goals are not a central part of its mission. In general, food hardships fall as food spending rises. WIC’s monthly food package effectively supplements household food budgets, increasing participants’ resources to buy food and potentially improving food security.[84]
Relatively few studies have looked directly at the relationship between WIC and food security. There is some indication, however, that participation in WIC is associated with improvements in food security, especially among children. One study estimates that participation in WIC reduces the prevalence of food insecurity among children by at least 20 percent.[85] In addition, indirect evidence of WIC’s impact is found in increases in food insecurity among children who age out of WIC after their fifth birthday but have not yet enrolled in kindergarten so do not receive free or reduced-price meals at school.[86] And among the most at-risk mothers in Massachusetts, the risk of household food insecurity after giving birth was about one-third lower if they enrolled in WIC in the first trimester of their pregnancy rather than the third.[87]
Impacts on Immunization, Health, and Cognitive Development
Low-income children participating in WIC have immunization rates comparable to more affluent children and significantly higher than low-income children who never participated — and are more likely to receive preventive medical care than other low-income children. Participation in WIC may also help reduce childhood obesity and reduce the prevalence of anemia. In addition, new evidence suggests that early exposure to WIC may improve children’s educational prospects.
-
WIC helps ensure that children are properly immunized. Immunizing children against disease is important to help them stay healthy and to protect others from diseases that once injured or killed thousands of children. Because of advances in medical science, immunized children are protected against more diseases than ever before. Widespread immunization also helps protect those who are too young or unable to be vaccinated. And by reducing, and in some cases eliminating, harmful diseases, today’s vaccinations can protect future generations from harm.
As an adjunct to health care services, WIC screens the immunization records of all infants and children under age 2 and refers parents to immunization services to help ensure that coverage is up to date. A recent study of families enrolled in Medicaid in South Carolina found that WIC participation was associated with a modest increase in the probability that an infant is vaccinated.[88]
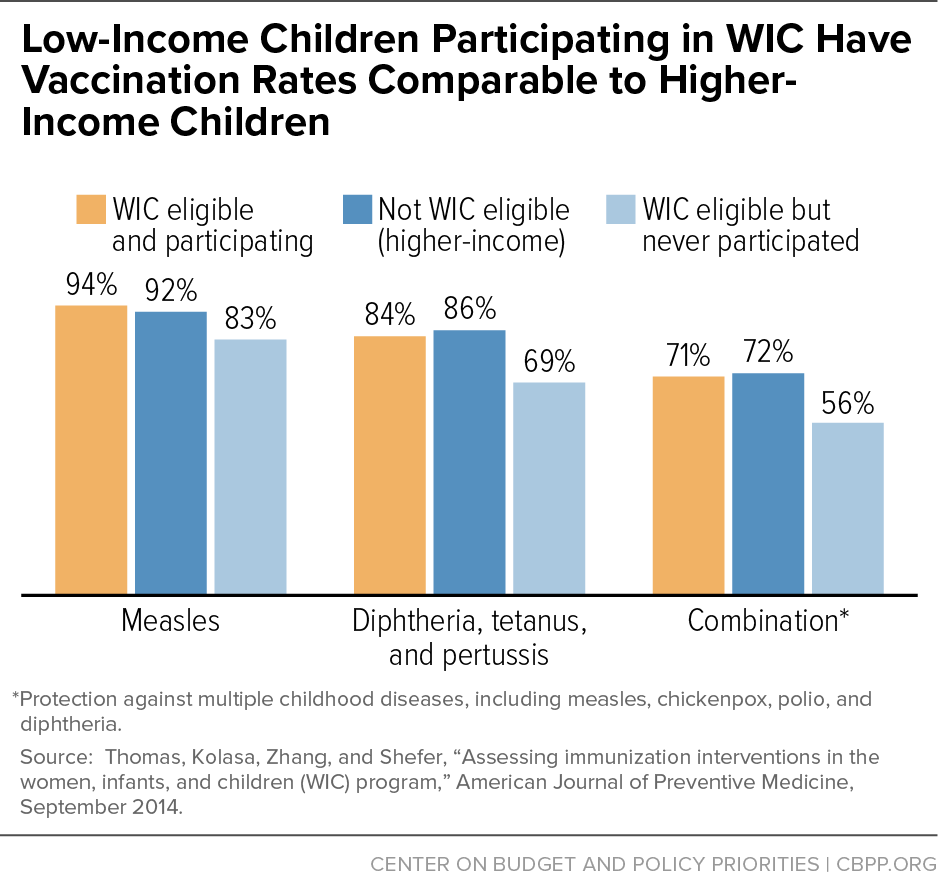
The findings are more striking for children. Low-income children who have never participated in WIC have immunization rates ranging from 5 to 19 percent lower than current participants, while children who remain in WIC tend to have immunization coverage comparable to higher-income children.[89] (See Figure 7.)
-
WIC improves access to health care. Children’s health depends partially on their access to health care services. Parents and children with access to health care are diagnosed and treated promptly and can obtain quality preventive care, which can enable them to avoid illness or complications. WIC serves as a gateway to health care, connecting families to resources such as prenatal, obstetric, maternal, and pediatric care; dental care; and counseling for smoking cessation drug and alcohol abuse. Recent USDA-sponsored research following mothers and children who enrolled in WIC as infants shows that nearly all (95 percent) have a doctor’s office, health clinic, or other medical facility that they visit for routine physical examinations and wellness checks by the time their child nears his or her fourth birthday.[90]
In general, research has shown that children who participate in WIC — or whose mothers do — make more use of health care services than non-participants. Researchers in North Carolina, for example, concluded that WIC participation among children was associated with increased use of preventive care and increased diagnosis and treatment of common childhood illnesses. Similar results regarding the frequency of well-child visits were found in a survey of unmarried, low-income urban mothers in 20 cities nationwide and in an analysis of Medicaid records in South Carolina.[91] Infants and children who participate in WIC are linked to the health care system and are much more likely to receive both preventive and curative care.
-
WIC may help reduce childhood obesity. The prevalence of childhood obesity in the United States more than tripled over the last four decades. One in five children were overweight or obese in 2016. Childhood obesity is particularly troubling because it is a strong predictor of adult obesity and can start children on the path to health problems previously confined to adults, such as diabetes, high blood pressure, and high cholesterol. There is reason to think that early intervention is important: the prevalence of obesity increases throughout early childhood and levels off by around age 10.[92]
WIC can reduce the risk of obesity among young children in several ways. Revised food packages provide fewer calories for most participants. The fruits, vegetables, and whole grains in the food package are consistent with recommended food patterns associated with healthy weight. In addition, rising breastfeeding rates among participating mothers may protect against excessive weight gain.
While evidence of overall progress in preventing obesity prevention in recent years is mixed, there are some hopeful signs of progress among young, low-income children. The prevalence of obesity among all children age 2 to 5 years was on a downward trend between 2004 and 2014, falling from 13.9 percent to 9.4 percent, before increasing back to 13.9 percent in 2016.[93] Obesity rates among low-income children enrolled in WIC, however, fell from 15.9 percent in 2010 to 13.9 percent in 2016, with significant decreases in all age, sex, and racial/ethnic subgroups. Obesity rates among WIC children fell in 36 states, the District of Columbia, and four territories over this period.[94]
-
WIC helps reduce the prevalence of anemia. Iron is an essential mineral that, among other functions, carries oxygen throughout the body and helps muscles store and use that oxygen. Iron deficiency anemia, resulting from too little iron in the body, can increase the risk of premature birth, delay normal motor skills and cognitive processing in infants, and cause fatigue or memory loss in adolescents and adults. In addition, the American Academy of Pediatrics notes that iron deficiency without anemia during infancy and childhood can have lasting implications for development and behavior.[95] While the nutrient intakes of infants, toddlers, and young children generally meet or exceed dietary recommendations, there is evidence of a subset of older infants whose iron intake falls short of those recommendations.[96]
WIC was created, in part, to reduce the prevalence of iron deficiency and iron deficiency anemia by providing only iron-fortified infant formulas, infant foods, and breakfast cereals in prescribed food packages for infants and young children. It may also have had an indirect effect, as manufacturers brought iron-fortified products reformulated for WIC to market, making them available to all children, whether they participate in WIC or not.
The evidence suggests that WIC played a role in reducing the prevalence of childhood anemia. CDC researchers found a steady decline in the prevalence of anemia between 1976 and 1985 (from 7.8 percent to 2.9 percent) and a reduction of more than 5 percent between 1980 and 1995, periods of substantial growth in WIC participation.[97] In addition, several studies have found that participation in WIC is associated with increased iron intake.[98] Most recently, data from a national survey of infant and toddler feeding practices show that the risk of inadequate iron intake among older infants (i.e., those between 6 and 12 months) is substantially lower in WIC participants (13 percent) compared with either lower-income (26 percent) or higher-income (34 percent) non-participants.[99]
-
Children who participate in WIC do better in school. There is substantial evidence that disadvantages during critical periods of brain development can affect children’s cognitive development and readiness to learn, producing disparities in skills and academic achievement. These disparities may grow as children age. WIC supports sound nutrition during critical periods of cognitive development to mitigate the detrimental effects of poverty.
Research suggests that prenatal and early childhood participation in WIC is associated with improved cognitive development and academic achievement. WIC is quite effective in reaching women during, rather than after, their pregnancy: 83 percent of new mothers participating in WIC enrolled during their pregnancy.[100] Children whose mothers participated in WIC while pregnant scored higher on assessments of mental development at age 2 than similar children whose mothers did not participate. The benefit associated with WIC participation persisted into the school years, as children whose mothers participated in WIC when they were in utero performed better on reading assessments.[101]
A more recent study in South Carolina associated prenatal WIC participation with a 5 percent reduction in the incidence of Attention-Deficit/Hyperactivity Disorder and other common childhood mental health conditions. Children whose mothers participated in WIC during pregnancy were also 8 percent less likely to repeat a grade. Since mental health problems are one of the causes of grade repetition, WIC might reduce grade repetition by improving children’s mental health. The effects were concentrated among Black children and the poorest Medicaid recipients — groups at high risk of negative birth outcomes.[102]
Impacts on Neighborhood Food Environments
Improvements to the WIC food packages and requirements that participating stores stock a wider array of more nutritious foods have helped create healthier neighborhood food environments, improving access to fruits, vegetables, and whole grains for many low-income communities.[103]
The environments in which people make food choices can affect their diet quality and health.[104] For some, eating a healthy diet may be difficult because nutritious options are not readily available, easily accessible, or affordable in their communities. Many low-income and underserved communities have few stores that sell healthy food, especially high-quality fruits and vegetables.[105] Limited availability of healthy foods can increase the risk of poor nutrition and chronic health conditions.
Revisions to the WIC food packages helped reshape the food retailing landscape in many communities. To obtain authorization to accept WIC food vouchers, stores must meet minimum food inventory requirements established by states.[106] As a result of the food package revisions, all WIC-authorized grocery stores must now stock at least two varieties of fruits, two varieties of vegetables, and at least one whole-grain cereal, potentially increasing their availability for all consumers.
Although participants obtain most of their WIC foods in large superstores, supermarkets, or grocery stores (76 percent in 2012), small grocery, convenience, and corner stores are important to the overall food environment in many neighborhoods.[107] The latest generation of research strongly suggests that the new requirements increased access to healthy foods in these smaller stores, especially in low-income communities. Multiple studies, conducted in various locations using different study designs, have consistently found that availability of healthy foods increased after implementation. For example:
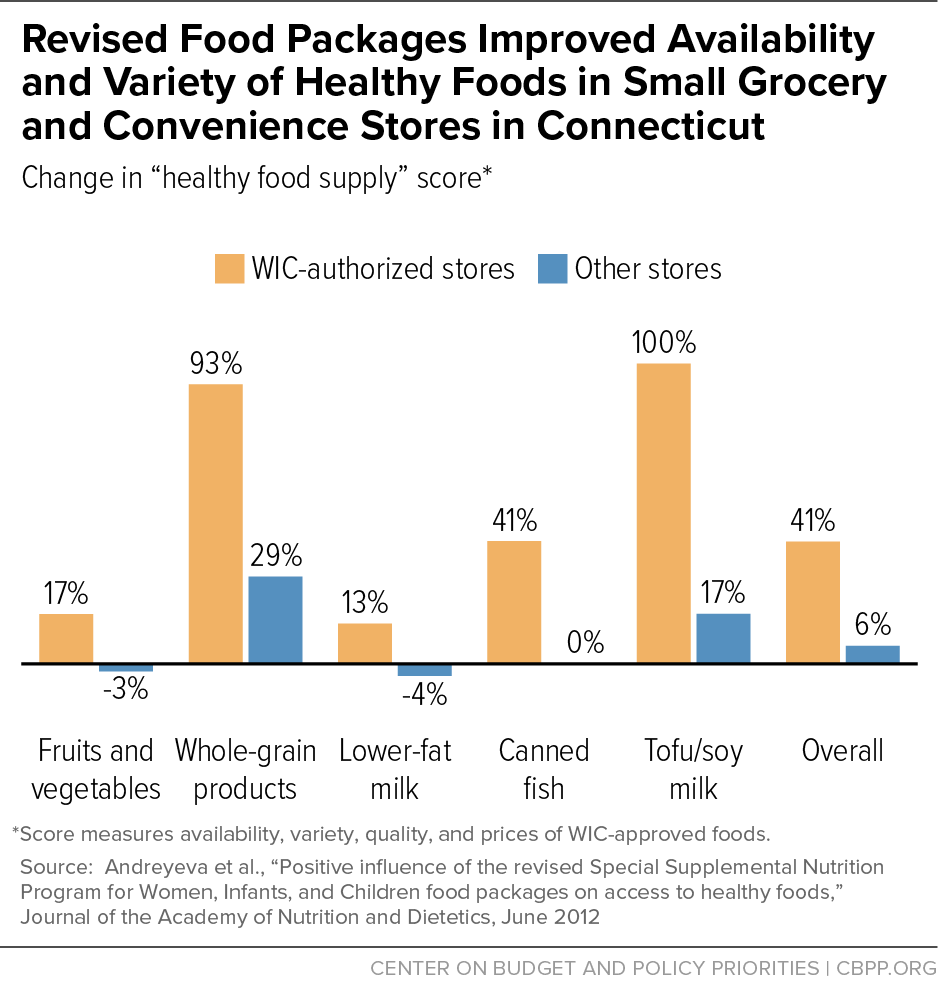
- Within months of implementation, WIC-approved convenience and grocery stores in Connecticut, especially those in low-income areas, offered more and a wider variety of healthy foods, especially whole-grain products.[108] (See Figure 8.)
- In two low-income neighborhoods in Philadelphia, the availability of reduced-fat milk, whole-grain bread, brown rice, 100-percent juice, and varieties of fruits and vegetables increased after implementation.[109]
- While supermarkets and larger grocery stores were likely to carry a wide range of healthy foods prior to the policy change, a natural experiment in New Orleans found large and significant increases in the percentage of small stores that carried nutritious foods, such as whole-wheat bread and brown rice.[110]
- The availability of commonly consumed fresh fruit and vegetables increased in WIC-approved stores in seven northern Illinois counties after introduction of the revised food packages.[111]
- The availability of fruits, vegetables, and whole grains in small stores across Colorado, New Hampshire, Pennsylvania, and Wisconsin increased significantly after implementation. The availability of low-fat (1 percent) milk increased in New Hampshire and Wisconsin, which did not allow participants to purchase reduced-fat (2 percent) milk.[112]
- The availability of healthy food improved significantly between 2006 and 2012 in 118 Baltimore food stores, with the greatest increases in corner stores and in predominately Black neighborhoods.[113]
- A review of 105 WIC-authorized stores in Texas documented increased shelf space and greater visibility of healthy foods between 2009 and 2012.[114]
Authorization to accept WIC benefits also has advantages for retailers, particularly smaller stores that may be the only easily accessible food store in some low-income communities. Recent research took advantage of a natural experiment in which one national discount variety store chain often located in low-income neighborhoods became an authorized WIC vendor in eight pilot stores in North Carolina. Researchers found that becoming a WIC vendor led to an increase in sales of healthy, WIC-eligible foods compared to similar stores not authorized as WIC vendors. In addition to an increase in sales volume of WIC-eligible foods, average weekly dollar sales per store increased by 15 percent.[115]
There is some evidence that the retail shopping experience of WIC participants could be improved. Interviews with a small number of WIC participants in four states revealed that many felt that identifying WIC-eligible items was sometimes challenging due to limited or inconsistent signage in retail stores. Most participants also reported feeling stigmatized by store employees and customers, particularly during checkout when they encountered delays while using WIC benefits.[116]
Conclusion
Research shows that poverty and adversity during early childhood can have lifelong consequences for physical, mental, and economic well-being. WIC is designed to support sound nutrition and health at critical points in children’s development — in utero, during infancy, and during the toddler and early childhood years. An extensive body of research over more than four decades shows that WIC participation is associated with healthier births, reduced infant mortality, better infant-feeding practices, more nutritious diets, better access to primary and preventive health care, and improved cognitive development and academic achievement. These striking results highlight the importance of ensuring that all eligible women and young children can get WIC benefits during pregnancy and critical periods of child development.
Are WIC’s Impacts Underestimated?
WIC originated with the desire to improve participants’ health and nutrition, but its benefits may reach further; a complete accounting of WIC’s effectiveness should capture the full range of direct and indirect benefits. Some of the beneficial consequences of WIC participation have not been fully measured, in part because they are not easily assessed with the methods available to today’s researchers. Many analysts have pointed to a variety of factors that may independently affect WIC’s impact and could also plausibly be affected by participation in WIC. For example,
- Controlling for early initiation of prenatal care may help account for differences between WIC participants and non-participants in the importance that mothers place on obtaining early health care during their pregnancy. But getting mothers into early prenatal care may be one way WIC improves birth outcomes.
- Controlling for gestational age may help account for the fact that longer gestation is linked to both healthier outcomes and more opportunities to enroll in WIC. But it comes at the cost of omitting improvements in gestational age that result from WIC participation.
- Controlling for smoking and drug use may help account for differences in the prevalence of risky behaviors among mothers. But smoking cessation counseling and referrals to substance abuse programs may be one way WIC leads to better birth outcomes.
In assessing the non-experimental evidence of WIC’s effectiveness, it is important to consider the tradeoff between controlling too little and too much for factors that may affect both birth outcomes and WIC participation, or could be affected by WIC.
It is similarly difficult to disentangle the effects of WIC on health care costs. Connecting women and children to the health care system may increase short-term costs associated with the prevention, diagnosis, and treatment of disease. But underutilization of health care in early childhood can lead to more health problems — and costs — when children go undiagnosed and untreated. And if participation in WIC contributes to better birth outcomes and healthier babies, as the evidence reviewed here suggests it does, then WIC has the potential to reduce costs associated with hospitalization and post-natal care.a
WIC can also have economic ramifications, some of which extend beyond program recipients. There is some evidence, for example, that WIC participation among eligible children increased up to and during the Great Recession and then declined as the economy recovered.b Thus, WIC helps reduce economic hardships for millions of participants when the economy falters and unemployment rises. In addition, to the extent that WIC increases total food expenditures, WIC benefits the country’s farmers. USDA estimates that farmers received almost $1.3 billion from the sale of commodities used in producing the $4.6 billion in WIC retail food sales (after rebates) in fiscal year 2008. This amounts to a net addition of $331 million to farm revenues after accounting for the food purchases participants would have made without WIC.c
a In the mid-1990s, the General Accounting Office conducted a comprehensive meta-analysis of 17 studies that examined the impact of WIC on Medicaid costs. It concluded that prenatal WIC participation reduced post-partum medical costs in the first year by more than enough to offset the entire cost of the prenatal WIC program. Research conducted for USDA similarly concluded that every dollar spent on the prenatal component of WIC was associated with Medicaid savings during the first 60 days after birth, ranging from $1.77 to $3.13. While much has changed since these studies were conducted, more recent evidence illustrates the continued potential for realizing savings through WIC participation. A cost-benefit analysis of the program’s impact on preterm births in California estimated societal savings of $1.24 to $6.83 for every dollar spent on prenatal WIC in 2017. See Nianogo et al. (2019). Economic evaluation of California prenatal participation in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) to prevent preterm birth. Preventive Medicine, 124: 42-49.
b Jackson MI, Mayne P (2016). Child access to the nutritional safety net during and after the Great Recession: the case of WIC. Social Science and Medicine, 170:197207.
c Hanson K, Oliveira V (2009). Economic Linkages between the WIC Program and the Farm Sector, EB-12, Washington, DC: Economic Research Service, USDA.
Appendix: Assessing the Strength of Evidence
WIC is one of the most thoroughly studied federal programs. The extensive research literature on WIC provides strong evidence of its effectiveness but has certain limitations.[117] Three commonly cited limitations are that these studies: (1) are almost entirely non-experimental, based on statistical comparisons between those who received benefits and those who did not; (2) are subject to potential selection bias as a consequence; and (3) do not fully address the problem of gestational age bias.
-
Experimental versus non-experimental evidence. Some research methods provide better evidence than others. The “gold standard” for evaluating the effectiveness of a program or intervention is the randomized control trial, which is designed to minimize the risk that factors unrelated to the intervention or program benefit will influence the results. Randomized control trials entail a random assignment process (like tossing a coin) that places people into a treatment or control group. Researchers can accurately estimate the impact of program participation as the difference in outcomes between the treatment (program) and control groups because they were randomly selected from the same population, lived through the same shifting programmatic, economic, and social conditions, and differ only in their program experience.
However, randomized control trials are generally not feasible to evaluate WIC’s effectiveness for a number of reasons, including the ethical issues raised by withholding beneficial nutrition and health benefits from a random sample of low-income mothers and children. As a result, researchers rely on a variety of quasi- and non-experimental approaches.
-
Selection bias. In the absence of a randomized control trial, research results may be biased by the self-selection of low-income mothers and their children into WIC. If mothers who enroll in WIC are more able, more motivated, healthier, or have access to better health care than other mothers, then selection bias may lead researchers to mistakenly conclude that WIC is more effective than it really is. But if mothers who enroll in WIC are more disadvantaged, exhibit more risky behaviors, or are more likely to experience adverse birth outcomes than other mothers, then selection bias may lead to conclusions that WIC is less effective than it really is.
-
Gestational age bias. Women whose pregnancies last longer have better birth outcomes; they also have more opportunities to enroll in WIC. Thus, women whose pregnancies last longer may have better birth outcomes because of their longer pregnancies, not because of WIC. Some researchers argue that the strong association observed among prenatal WIC participation, birth weight, and the frequency of preterm births is largely spurious, the result of not controlling for gestational age bias. As a result, they focus on measures of fetal growth (such as birth weight adjusted for gestational age) and find positive but more modest associations with WIC participation.[119]
It is likely, however, that correcting for gestational age at birth may understate WIC’s positive impact on birth outcomes because it does not capture any positive effect WIC has on extending the duration of healthy pregnancies. An important study takes a different approach, using linked Medicaid and WIC records in California to compare women in each week of gestation. This approach addresses gestational age bias by comparing birth outcomes among women whose pregnancies reach the same length and who have the same opportunity to use WIC and concludes that participation is associated with large reductions in the risk of adverse birth outcomes.[120]
- Pre-natal survival bias. Some researchers have recently argued that more attention needs to be paid to the processes that affect which implanted pregnancies become live births, because the same mechanisms believed responsible for many of the lasting effects of early adversity are documented predictors of whether a healthy pregnancy is established and maintained. These researchers suggest that assuming prenatal selection is random, when in fact it is not, can produce a nontrivial bias that may mask the true effect of a program like WIC. The true effect of WIC, they speculate, may be substantially underestimated or not detected at all in the presence of this survival bias if program participation improves survival in the early stages of pregnancy.[121]
Our assessment acknowledges the valid evidential contribution of different research methods while giving greater weight to evidence generated from groups of studies across multiple populations, settings, and circumstances. While the research about WIC’s effectiveness may rely on methods that fall short of the “gold standard,” few public programs have so consistent a body of positive research findings.
End Notes
[1] Steven Carlson is a research analyst who previously directed the Office of Policy Support at the Agriculture Department’s Food and Nutrition Service. The opinions and conclusions expressed in this report are solely those of the authors and should not be construed as representing the views of the Agriculture Department.
[2] For more information on how WIC operates, see Policy Basics: Special Supplemental Nutrition Program for Women, Infants, and Children, Center on Budget and Policy Priorities, updated April 26, 2017, https://www.cbpp.org/cms/index.cfm?fa=view&id=5268.
[3] Fox MK, Hamilton W, Lin BH, eds., (2004). Effects of Food Assistance and Nutrition Programs on Nutrition and Health: Volume 3, Literature Review. Food Assistance and Nutrition Research Report No. 19-3, U.S. Department of Agriculture, Economic Research Service, https://www.ers.usda.gov/webdocs/publications/fanrr193/30219_fanrr19-3fm_002.pdf; Colman S, Nichols-Barrer IP, Redline JE, Devane BL, Ansell SV, and Joyce T (2012). Effects of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC): A Review of Recent Research. Report WIC-12-WM. U.S. Department of Agriculture, Food and Nutrition Service, https://www.fns.usda.gov/effects-special-supplemental-nutrition-program-women-infants-and-children-wic-review-recent-research.
[4] See, for example, Brooks-Gunn J, Duncan G (1997). The effects of poverty on children. The Future of Children 7(2). For a comprehensive review of more recent evidence that children growing up in poor families fare worse than children in more affluent families, see Duncan G, Le Menestrel, eds., (2019). A Roadmap to Reducing Child Poverty. Washington, DC: The National Academies Press.
[5] Cook JT, Frank DA (2008). Food security, poverty, and human development in the United States. Annals of the New York Academy of Sciences, 1136(1):193-209. Food insecurity is defined as lack of access to a safe and secure source of enough food to sustain an active, healthy life.
[6] Halfon N et al (2020). Measuring equity from the start: disparities in the health development of US kindergartners. Health Affairs, 39(10): 1702-1709.
[7] Currie J, RossinSlater M (2015). Earlylife origins of lifecycle wellbeing: research and policy implications. Journal of Policy Analysis and Management, 34(1):208242; Center on the Developing Child at Harvard University (2016). From Best Practices to Breakthrough Impacts, https://developingchild.harvard.edu/wp-content/uploads/2016/05/From_Best_Practices_to_Breakthrough_Impacts-4.pdf, accessed on August 8, 2020; and Duncan and Le Menestrel (2019), op cit.
[8] Center on the Developing Child at Harvard University (2010). The foundations of lifelong health are built in early childhood, http://www.developingchild.harvard.edu/, accessed on December 5, 2014.
[9] Duncan GJ, Magnuson K, Kalil A, Ziol-Guest K (2012). The importance of early childhood poverty. Social Indicators Research 108:87-98.
[10] Ratcliffe C, McKernan SM (2012). Child Poverty and Its Lasting Consequence. Low-Income Families Working Paper 21, Washington, DC: The Urban Institute, http://www.urban.org/research/publication/child-poverty-and-its-lasting-consequence.
[11] Nelson BB et al. (2016). Predictors of poor school readiness in children without developmental delay at age 2. Pediatrics, 138(2), http://pediatrics.aappublications.org/content/pediatrics/138/2/e20154477.full.pdf.
[12] Duncan GJ, Magnuson K, Votruba-Drzal E (2017). Moving beyond correlations in assessing the consequences of poverty. Annual Review of Psychology, 68:413-434.
[13] Duncan GJ, Ziol-Guest K, Kalil A (2010). Early-childhood poverty and adult attainment, behavior, and health. Child Development, 81(1):306-325. The authors estimate that a $10,000 annual increase in low-income families’ income before a child’s fifth birthday is associated with a 68 percent increase in adult earnings and more than 500 additional work hours per year after age 25.
[14] Blair C, Raver C (2016). Poverty, stress, and brain development: New directions for prevention and intervention. Academic Pediatrics, 16(3), S30-S36.
[15] Shonkoff J, Garner A, Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, and Section on Developmental and Behavioral Pediatrics (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129(1):e232-246.
[16] Early life experiences may also affect nutrition behavior later in life. A recent systematic review identified a 46 percent increase in the odds of adult obesity following exposure to multiple adverse events in childhood. See Wiss DA, Brewerton TD (2020). Adverse childhood experiences and adult obesity: a systematic review of plausible mechanisms and meta-analysis of cross-sectional studies. Physiology & Behavior, 223(1):112964. A study of adults in Nevada suggests that fruit and vegetable consumption in adulthood may also be associated with the cumulative effects of multiple adverse childhood experiences. See Horino M, Yang W (2020). Impact of adverse childhood experiences and fruit and vegetable intake in adulthood. Public Health Nutrition, published online April 22.
[17] Cameron AJ, Spence AC, Laws R, Hesketh KD, Lioret S, Campbell K J (2015). A review of the relationship between socioeconomic position and the early-life predictors of obesity. Current Obesity Reports, 4(3):350-362.
[18] Wen X, Kong KL, Eiden RD, Sharma NN, Xie C (2014). Sociodemographic differences and infant dietary patterns. Pediatrics, 134(5):e1387-1398, https://www.researchgate.net/profile/Kai_Ling_Kong2/publication/266948125_Sociodemographic_Differences_and_Infant_Dietary_Patterns/links/55312b5c0cf27acb0dea690f.pdf.
[19] Grummer-Strawn LM, Li R, Perrine CG, Scanlon KS, Fein SB (2014). Infant feeding and long-term outcomes: results from the year 6 follow-up of children in the Infant Feeding Practices Study II. Pediatrics, 134 (Supplement 1):S1-S3.
[20] Devaney B (1992). Very Low Birthweight among Medicaid Newborns in Five States: The Effects of Prenatal WIC Participation. Alexandria, Virginia: Food and Nutrition Service, USDA; Devaney B, Bilheimer L, Schore J (1990). The Savings in Medicaid Costs for Newborns and Their Mothers from Prenatal WIC Participation in the WIC Program, Volume 1. Alexandria, VA: Food and Nutrition Service, USDA; Devaney B, Bilheimer L, Schore J (1991). The Savings in Medicaid Costs for Newborns and Their Mothers from Prenatal WIC Participation in the WIC Program, Volume 2. Alexandria, VA: Food and Nutrition Service, USDA; Devaney B, Schirm A (1993). Infant Mortality among Medicaid Newborns in Five States: The Effects of Prenatal WIC Participation. Alexandria, VA: Food and Nutrition Service, USDA. In light of the significant changes in the WIC and Medicaid participation and policy environments, USDA launched a second WIC-Medicaid Study in 2010. The study’s goal was to use linked administrative data from WIC, Medicaid, and vital records in two states (Missouri and Oklahoma) to assess the feasibility of examining the association between WIC participation during pregnancy and early childhood and birth outcomes and health care utilization and costs. While the project demonstrated the feasibility of this approach to analyze WIC’s impact on an expanded set of pregnancy and birth outcomes, the absence of cost data for the growing number of Medicaid recipients in managed care programs presented an unsurmountable challenge to measuring the association between WIC and Medicaid costs. See Kranker K, Fox MK, Caronongan P (2018). WIC−Medicaid II Feasibility Study: Final Report, Alexandria, VA: Food and Nutrition Service, USDA.
[21] This review, sponsored by USDA’s Economic Research Service, points out that “the consistency of the results across studies is noteworthy. This is especially true when . . . the bulk of the literature is comprised of relatively large, well-conducted studies, [and] includes both national samples and state-level data . . . from a number of different time periods” (Fox Hamilton and Lin (2004) op. cit.).
[22] Colman et al., op. cit.
[23] Hamad R, Collin DF, Bae, RJ, Jelliffe-Pawlowski LL (2019). Association of revised WIC food package with perinatal and birth outcomes: a quasi-experimental study. JAMA Pediatrics, 173(9): 845-852.
[24] Blakeney EL, Herting JR, Zierler BK, Bekemeier B (2020). The effect of women, infant, and children (WIC) services on birth weight before and during the 2007–2009 great recession in Washington state and Florida: a pooled cross-sectional time series analysis. BMC Pregnancy and Childbirth, 20: 1-13.
[25] See, for example, Lazariu-Bauer V, Stratton H, Pruzek R, Woelfel ML (2004). A comparative analysis of effects of early versus late prenatal WIC participation on birth weight: NYS, 1995. Maternal and Child Health Journal, 8(2):77-86; Bitler MP, Currie J (2005).
Does WIC work? The effects of WIC on pregnancy and birth outcomes. Journal of Policy Analysis and Management, 24(1):73-91; Joyce T, Gibson D, Colman S (2005). The changing association between prenatal participation in WIC and birth outcomes in New York City. Journal of Policy Analysis and Management, 24(4):661-685; Joyce T, Racine A, Yunzal-Butler C (2008). Reassessing the WIC effect: evidence from the pregnancy nutrition surveillance system. Journal of Policy Analysis and Management, 27(2):277-303; Hoynes HW, Page ME, Stevens AH (2011). Can targeted transfers improve birth outcomes? Evidence from the introduction of the WIC program. Journal of Public Economics, 95(7):813-827; and Rossin-Slater M (2013). WIC in your neighborhood: new evidence on the impacts of geographic access to clinics. Journal of Public Economics, 102:51-69.
[26] These increases are likely to be clinically relevant. “Small WIC impacts on birth outcomes may be sufficient for program benefits to exceed costs, given the relatively modest program costs per pregnant mother and the substantial medical and other social savings associated with averting even a small number of poor birth outcomes” (Ludwig J Miller M (2005). Interpreting the WIC debate. Journal of Policy Analysis and Management 24(4):691-701.)
[27] Bitler and Currie (2005), op. cit.
[28] Joyce et al. (2008), op. cit.; Currie J, Rajani I (2014). Within-mother estimates of the effects of WIC on birth outcomes in New York City. Working Paper 20400, Cambridge, MA: National Bureau of Economic Research; Sonchak L (2016). The impact of WIC on birth outcomes: new evidence from South Carolina. Maternal and Child Health Journal, 20(7):15181525; and Chorniy A, Currie J, Sonchak L (2020). Does prenatal WIC participation improve child outcomes? American Journal of Health Economics, 6(2): 169-198. In addition, the last reference cited here suggests that WIC may have larger effects on more disadvantaged mothers who are at higher risk of adverse birth outcomes. The WIC-Medicaid II Feasibility Study found no evidence of WIC’s impact on birthweight in Missouri or Oklahoma (Kranker, Fox, and Caronongan (2018) op. cit.).
[29] Fingar KR, Lob SH, Dove MS, Gradziel P, Curtis MP (2016). Reassessing the association between WIC and birth outcomes using a fetusesatrisk approach. Maternal and Child Health Journal, 21(4), 825-835.
[30] Kranker, Fox, and Caronongan (2018) op. cit. These researchers note that the estimated reductions in the probability of preterm birth obtained from their approach (using discrete time hazard models) are smaller than those estimated in previous research that did not adjust for gestational-age bias. They suggest that the difference in average gestational lengths between WIC participants and non-participants is, to a large extent, driven by gestational-age bias (not impacts of WIC on gestational age).
[31] There is also some limited evidence that WIC participation may be associated with reductions in the risk of pregnancies that end with a stillbirth among non-Hispanic Black women. See Angley M et al. (2018). Association of participation in a supplemental nutrition program with stillbirth by race, ethnicity, and maternal characteristics. BMC Pregnancy and Childbirth, 18(1): 306.
[32] See, for example, the summary in Table 18 of USDA, Economic Research Service (2004). More recently, however, the WIC-Medicaid II feasibility study found no impact of WIC on infant mortality in Missouri and Oklahoma (Kranker, Fox and Caronongan (2018) op. cit.).
[33] Soneji S, Beltrán-Sánchez H (2019). Association of Special Supplemental Nutrition Program for Women, Infants, and Children with preterm birth and infant mortality. JAMA Network Open, 2(12): e1916722-e1916722.
[34] Khanani I, Elam J, Hearn R, Jones C, Maseru N (2010). The impact of prenatal WIC participation on infant mortality and racial disparities. American Journal of Public Health, 100(Supplement 1):S204-S209.
[35] Keene-Woods N, Reyes J, Chesser A (2016). Infant mortality and race in Kansas: associations with women, infants, and children services. Journal of Primary Care and Community Health, 7(3):194198, http://journals.sagepub.com/doi/pdf/10.1177/2150131916635572.
[36] Li R, Dee D, Li CM, Hoffman HJ, Grummer-Strawn LM (2014). Breastfeeding is associated with reduced risk of infections at age 6 years. Pediatrics, 134(Supplement 1):S13–S20; Pan L, Li R, Park S, Galuska D, Sherry B, Freedman DS (2014). A longitudinal analysis of sugar-sweetened beverage intake during infancy and obesity at six years old. Pediatrics, 134(Supplement 1):S29–S35; Park S, Pan L, Sherry B, Li R (2014). A longitudinal analysis of sugar-sweetened beverage and 100% juice intake during infancy with sugar-sweetened beverage intake at six years old. Pediatrics, 134(Supplement 1):S56–S62; and Grimm KA, Kim SA, Yaroch AL, Scanlon KS (2014). Association of fruit and vegetable intake during infancy and early childhood. Pediatrics, 134(Supplement 1):S63–S69.
[37] On February 28, 2014, USDA released a final rule, replacing the interim rule issued in December 2007. The final rule raised the dollar amount for children’s fruit and vegetable purchases by more than 30 percent. It also expanded whole-grain options available to participants, provided yogurt as a partial milk substitute for women and children, allowed parents of older infants to purchase fresh fruits and vegetables instead of jarred infant food if they choose, and gave state and local agencies more flexibility to meet the nutritional and cultural needs of participants.
[38] National Academies of Sciences, Engineering, and Medicine (2017). Review of WIC Food Packages: Improving Balance and Choice (Final Report). Washington, DC: The National Academies Press, https://www.nap.edu/catalog/23655/review-of-wic-food-packages-improving-balance-and-choice-final. USDA has not acted on these recommendations as of this writing. USDA and HHS released the Scientific Report of the 2020 Dietary Guidelines Advisory Committee to the Secretaries of USDA and HHS (the basis for forthcoming 2020 Dietary Guidelines) in July 2020.
[39] Colman et al. (2012) op. cit.
[40] Au LE, Gurzo K, Paolicelli C, Whaley SE, Weinfield NS, Ritchie LD (2018). Diet quality of US infants and toddlers 7–24 months old in the WIC Infant and Toddler Feeding Practices Study-2. The Journal of Nutrition, 148(11):1786-1793. The HEI is a measure of diet quality used to assess how well a set of foods aligns with key recommendations of the Dietary Guidelines for Americans. An HEI score of 100 indicates that an individual has consumed at least the recommended daily values of 10 dietary components.
[41] Weinfield NS, Borger C, Au LE, Whaley SE, Berman D. Ritchie LD (2020). Longer participation in WIC is associated with better diet quality in 24-month-old children. Journal of the Academy of Nutrition and Dietetics, 120(6), 963-971; Au LE, Paolicelli C, Gurzo K, Ritchie LD, Weinfield NS, Plank KR, Whaley SE (2019). Contribution of WIC-eligible foods to the overall diet of 13-and 24-month-old toddlers in the WIC Infant and Toddler Feeding Practices Study-2. Journal of the Academy of Nutrition and Dietetics, 119(3): 435-448.
[42] Borger C et al. (2020). WIC Infant and Toddler Feeding Practices Study-2 Fourth Year Report. Prepared by Westat, Inc. for USDA Food and Nutrition Service, September.
[43] This analysis also suggests that the improvements in nutritional quality are not simply a reflection of unobserved differences between participants and non-participants. WIC households had healthier purchases only when benefits were redeemed. During weeks when benefits were not redeemed, the nutritional quality of purchases among WIC households was no different from that of eligible non-participating households. In addition, among those redeeming WIC benefits, the improvements in purchase quality disappeared once shopping baskets filled mainly with WIC-eligible foods were excluded from the analysis. Taken together, the evidence suggests that foods provided by WIC can explain most if not all of the improvement in the quality of food purchases. See Fang D, Thomsen MR, Nayga RM, Novotny AM (2019). WIC participation and relative quality of household food purchases: Evidence from FoodAPS. Southern Economic Journal, 86(1), 83-105.
[44] Khan R, Zhu T, Dhar S (2018). The effect of the WIC program on consumption patterns in the cereal category. Quantitative Marketing and Economics, 16(1): 79-109.
[45] Schultz DJ, Byker Shanks C, Houghtaling B (2015). The impact of the 2009 Special Supplemental Nutrition Program for Women, Infants, and Children food package revisions on participants: A systematic review. Journal of the Academy of Nutrition & Dietetics, 115:1832–46; Zhang Q, Alsuliman MA, Wright M, Wang Y, Cheng X (2020). Fruit and vegetable purchases and consumption among WIC participants after the 2009 WIC food package revision: a systematic review. Advances in Nutrition, published online May 26.; Hartline-Grafton H (2019). Impact of the Revised WIC Food Packages on Nutrition Outcomes and the Retail Food Environment. Food Research and Action Center, https://frac.org/wp-content/uploads/frac_brief_revised_wic_food_package_impact_nutrition_retail.pdf.
[46] Zhang et al., op. cit.
[47] Whaley SE, Ritchie LD, Spector P, Gomez J (2012). Revised WIC food package improves diets of WIC families. Journal of Nutrition Education and Behavior, 44(3):204-209.
[48] Andreyeva T, Luedicke J (2014). Incentivizing fruit and vegetable purchases among participants in the Special Supplemental Nutrition Program for Women, Infants, and Children. Public Health Nutrition, 1-9; Andreyeva T, Luedicke J (2013). Federal food package revisions: effects on purchases of whole-grain products. American Journal of Preventive Medicine, 45(4):422-429; Andreyeva T, Luedicke J, Tripp AS, Henderson KE (2013). Effects of reduced juice allowances in food packages for the women, infants, and children program. Pediatrics, 131(5):919-927; Andreyeva T, Luedicke J, Henderson KE, Schwartz MB (2014). The positive effects of the revised milk and cheese allowances in the special supplemental nutrition program for women, infants, and children. Journal of the Academy of Nutrition and Dietetics, 114(4):622-630.
[49] Chiasson MA, Findley SE, Sekhobo JP, Scheinmann R, Edmunds LS, Faly AS, McLeod NJ (2013). Changing WIC changes what children eat. Obesity, 21(7): 1423-1429.
[50] Ng SW, Hollingsworth BA, Busey EA, Wandell JL, Miles DR, Poti JM (2018). Federal nutrition program revisions impact low-income households’ food purchases. American Journal of Preventive Medicine, 54(3): 403-412.
[51] Meiqari L, Torre L, Gazmararian JA (2015). Exploring the impact of the new WIC food package on lowfat milk consumption among WIC recipients: a pilot study. Journal of Health Care for the Poor and Underserved, 26(3):712725.
[52] Odoms-Young AM, Kong A, Schiffer LA, Porter SJ, Blumstein L, Bess S, Berbaum ML, Fitzgibbon ML (2014). Evaluating the initial impact of the revised Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food packages on dietary intake and home food availability in African-American and Hispanic families. Public Health Nutrition, 17(1): 83-93.
[53] Kong A, Odoms-Young AM, Schiffer LA, Kim Y, Berbaum ML, Porter SJ, Blumstein L, Bess S, Fitzgibbon ML (2014). The 18-month impact of special supplemental nutrition program for women, infants, and children food package revisions on diets of recipient families. American Journal of Preventive Medicine, 46(6): 543-551.
[54] Ishdorj A, Capps O (2015). Rural vs. urban Texas WIC children food choices and intakes before and after changes in the food benefits. Department of Agricultural Economics, Texas A&M University; and Ishdorj A, Capps O (2013). The effect of revised WIC food packages on Native American children. American Journal of Agricultural Economics, 95(5):1266-1272.
[55] Tester JM, Leung CW, Crawford PB (2016). Revised WIC food package and children’s diet quality. Pediatrics, 137(5):e20153557 .
[56] Chaparro MP, Crespi CM, Anderson CE, Wang MC, Whaley SE (2019). The 2009 Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food package change and children's growth trajectories and obesity in Los Angeles County. The American Journal of Clinical Nutrition, 109(5):1414-1421. Subsequent studies by the same research team suggest that the WIC food package changes may not have benefited all children equally: obesity reduction was weaker for girls in some circumstances. See Chaparro MP, Anderson CE, Crespi CM, Whaley SE, Wang MC (2019). The effect of the 2009 WIC food package change on childhood obesity varies by gender and initial weight status in Los Angeles County. Pediatric Obesity, 14(9):e12526; Anderson CE, Crespi CM, Wang MC, Whaley SE, Chaparro MP (2020). The neighborhood food environment modifies the effect of the 2009 WIC food package change on childhood obesity in Los Angeles County, California. BMC Public Health, 20: 1-11.
[57] Chaparro MP, Wang MC, Anderson CE, Crespi CM, Whaley SE (2020). The association between the 2009 WIC food package change and early childhood obesity risk varies by type of infant package received. Journal of the Academy of Nutrition and Dietetics, 120(3):371-385 and Chaparro MP, Anderson CE, Crespi CM, Wang MC, Whaley SE (2020). The new child food package is associated with reduced obesity risk among formula fed infants participating in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) in Los Angeles County, California, 2003–2016. International Journal of Behavioral Nutrition and Physical Activity, 17(1):18.
[58] Daepp MI, Gortmaker SL, Wang YC, Long MW, Kenney EL (2019). WIC food package changes: Trends in childhood obesity prevalence. Pediatrics, 143(50): e20182841.
[59] Oberle MM, Freese R, Shults J, Stallings VA, Virudachalam S (2020). Impact of the 2009 WIC food package changes on maternal dietary quality. Journal of Hunger & Environmental Nutrition, published online February 10.
[60] Section on Breastfeeding, American Academy of Pediatrics (2012). Breastfeeding and the use of human milk. Pediatrics, 129(3):e827-e841.
[61] Ip S, Chung M, Raman G, Chew P, Magula N, DeVine D, Trikalinos T, Lau J (2007). Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries. Evidence Report/Technology Assessment No. 153 (Prepared by Tufts-New England Medical Center Evidence-based Practice Center, under Contract No. 290-02-0022). AHRQ Publication No. 07-E007. Rockville, MD: Agency for Healthcare Research and Quality.
[62] See, for example, Zhang Q, Lamichhane R, Wright M, McLaughlin PW, Stacy B (2019). Trends in breastfeeding disparities in US infants by WIC eligibility and participation. Journal of Nutrition Education and Behavior, 51(2): 182-189.
[63] Gregory EF, Gross SM, Nguyen TQ, Butz AM, Johnson SB (2016). WIC participation and breastfeeding at 3 months postpartum. Maternal and Child Health Journal, 20(8):17351744.
[64] This study controlled for self-selection bias by focusing on mothers who gave birth after participating in WIC during one pregnancy but not a second. Each mother in this model essentially serves as her own control. Because the analysis is limited to mothers with multiple births and only those in South Carolina, the results may not apply to mothers with single births or to other parts of the country. See Sonchak L (2017). The impact of WIC on breastfeeding initiation and gestational weight gain: Case study of South Carolina Medicaid mothers. Children and Youth Services Review, 79:115-125.
[65] Centers for Disease Control and Prevention. Breastfeeding among U.S. children born 2002–2013, CDC National Immunization Survey accessed on February 6, 2017; Breastfeeding among U.S. children born 2010–2017, CDC National Immunization Survey available online at https://www.cdc.gov/breastfeeding/data/nis_data/results.html; accessed on September 12, 2020.
[66] Kline N, Thorn B, Bellows D, Wroblewska K. Wilcox-Cook E (2020). WIC Participant and Program Characteristics 2018. Prepared by Insight Policy Research for the Food and Nutrition Service, USDA (Appendix Table A.32). While these are the best data available, it is important to note that some of the increase in breastfeeding rates among women participating in WIC may be due to improved reporting over this period. In 2002, 68 state agencies reported WIC breastfeeding rates; by 2018 this had grown to 88 state agencies (covering 98 percent of all WIC participants). While the true increase between 2002 and 2018 may be somewhat smaller than reported, the growth in breastfeeding rates among WIC mothers still exceeds the national trend.
[67] Few studies examine the role of participants’ preference for and perceived value of WIC foods and packages in program participation and retention. Based on a survey and in-depth interviews of participants at eight WIC clinics in Illinois, researchers found that participants prioritized the infant packages over other WIC foods and packages, influenced by the high cost of infant formula. Weber S, Uesugi K, Greene H, Bess S, Reese L, and Odoms-Young A (2018). Preferences and Perceived Value of WIC Foods Among WIC Caregivers. Journal of Nutrition Education and Behavior, 50(7):695-704.
[68] Jacknowitz A Tiehen L (2010). WIC Participation Patterns: An Investigation of Delayed Entry and Early Exit. Economic Research Service, USDA, December, https://www.ers.usda.gov/webdocs/publications/44781/8018_err109.pdf?v=4458.5.
[69] Whaley SE, Whaley M, Au LE, Gurzo K, Ritchie LD (2017). Breastfeeding is associated with higher retention in WIC after age 1. Journal of Nutrition Education and Behavior, 49(10):810-816. Based on detailed discussions with a small number of WIC participants in Los Angeles, researchers speculate that mothers who formula-feed and predominantly receive material supports from WIC are less motivated to stay in the program after the formula benefits end, while breastfeeding mothers who receive both material and social supports feel more connected to WIC and are motivated to continue using WIC services even when material supports are reduced. See Almeida R, Gutierrez SA, Whaley SE, Ventura AK (2020). A qualitative study of breastfeeding and formula-feeding mothers’ perceptions of and experiences in WIC. Journal of Nutrition Education and Behavior, 52(6):615-625.
[70] Whaley SE, Martinez CE, Paolicelli C, Ritchie LD, Weinfield NS (2020). Predictors of WIC participation through 2 years of age. Journal of Nutrition Education and Behavior, 52(7): 672-679.
[71] As the committee’s report noted, “[a] breastfeeding mother — especially one who intends to combine breastfeeding and formula feeding, who needs to return to work, or who faces other personal challenges to breastfeeding — may need some formula to nourish her infant adequately during the first month postpartum. Some mothers who might otherwise try breastfeeding may choose formula feeding to be sure they can obtain formula (a high-cost item) if they run into breastfeeding difficulties.”
[72] This evaluation assessed initiation, intensity, and duration of breastfeeding. It also found that after the change, fewer WIC participants who were mothers of new infants received the partially breastfeeding package and more received the fully breastfeeding package, but more mothers also received the fully formula feeding package. Wilde P, Wolf A, Fernandez M, Collins A (2011). Evaluation of the Birth Month Breastfeeding Changes to the WIC Food Packages. Alexandria, VA: Food and Nutrition Service, USDA, https://www.fns.usda.gov/evaluation-birth-month-breastfeeding-changes-wic-food-packages.
[73] Rasmussen KM, Latulippe ME, Yaktine AL (2016). Review of WIC food packages: proposed framework for revisions (interim report). Food and Nutrition Board, Institute of Medicine, https://www.fns.usda.gov/wic/review-wic-food-packages-proposed-framework-revisions.
[74] Whaley SE, Koleilat M, Whaley M, Gomez J, Meehan K, Saluja K (2012). Impact of policy changes on infant feeding decisions among low-income women participating in the Special Supplemental Nutrition Program for Women, Infants, and Children. American Journal of Public Health, 102(12):2269-2273. It is possible that some of this increase was due to a successful breastfeeding promotion campaign for WIC participants and staff that began shortly before the introduction of the revised food packages. As noted above, Wilde et al. (2011) report a reduction in the number of mothers receiving the partial breastfeeding package but an increase in the number receiving the full-formula package in a random sample of 17 local WIC agencies.
[75] Langellier BA, Chaparro MP, Wang MC, Koleilat M, and Whaley SE (2014). The new food package and breastfeeding outcomes among women, infants, and children participants in Los Angeles County. American Journal of Public Health, 104(2):S112–S118.
[76] Thornton HE, Crixell SH, Reat AM, Von Bank JA (2014). Differences in energy and micronutrient intakes among central Texas WIC infants and toddlers after the package change. Journal of Nutrition Education and Behavior, 46(3 Supplement): S79-S86.
[77] Di H, Ishdorj A, McKyer L (2018). Impact of revised WIC food packages on infant feeding and transition to complementary foods. Presented at 2018 Agricultural and Applied Economics Association Annual Meeting, Washington, DC; and Ishdorj A, Di H, Samman E, McKyer ELJ (2020). Are rural infants benefiting from WIC food package rule changes? Breastfeeding and infant feeding behaviors. Southwest Rural Health Research Center.
[78] Li K, Wen M, Reynolds M, Zhang Q (2019). WIC participation and breastfeeding after the 2009 WIC revision: a propensity score approach. International Journal of Environmental Research and Public Health, 16(15):2645. The authors note that several earlier studies have found breastfeeding rates (initiation and duration) to be lower among WIC participants than eligible non-participants.
[79] At least one study, while observing that the rate at which children are ever breastfed increased across the nation, concluded that the increase is not associated with changes in the WIC food packages. See Joyce T, Reeder J (2015). Changes in breastfeeding among WIC participants following implementation of the new food package. Maternal and Child Health Journal, 19(4):868-876.
[80] Houghtaling B, Byker Shanks C, Jenkins M (2017). Likelihood of breastfeeding within the USDA’s Food and Nutrition Service Special Supplemental Nutrition Program for Women, Infants, and Children population: a systematic review of the literature. Journal of Human Lactation, 33(1): 83-97.
[81] Metallinos-Katsaras E, Brown L, Colchamiro R 2015. Maternal WIC participation improves breastfeeding rates: a statewide analysis of WIC participants. Maternal and Child Health Journal, 19(1):136-143.
[82] May L et al. (2017). WIC Infant and Toddler Feeding Practices Study – 2: Infant Year Report. Prepared by Westat, Inc., for the Food and Nutrition Service, USDA; Guthrie JF et al. (2018). WIC and non-WIC infants and children differ in usage of some WIC-provided foods. The Journal of Nutrition, 148 (Supplement 3): 1547S-1556S.
[83] Cook JT et al. (2013). Are food insecurity’s health impacts underestimated in the U.S. population? Marginal food security also predicts adverse health outcomes in young U.S. children and mothers. Advances in Nutrition: An International Review Journal, 4(1):51-61.
[84] We would expect WIC’s impact on food security to be relatively modest given the value of the monthly WIC food benefit — about $63 per person in fiscal year 2019. (Note that the average monthly cost to the federal government was much lower — about $41 — due to discounts on infant formula.) By way of comparison, the Supplemental Nutrition Assistance Program (food stamps) provided a monthly benefit of $130 per person in 2019.
[85] Kreider B, Pepper JV, Roy M (2016). Identifying the effects of WIC on food insecurity among infants and children. Southern Economic Journal, 82(4):1106-1122. More recent technical work suggests that participating in both SNAP and WIC may improve the food security rate by 24 percentage points compared with participating in SNAP alone. Because of the small sample used in this analysis, however, the positive impact could be as little as 1.9 percentage points. See Jensen HH, Kreider B, Zhylyevskyy O (2019). Investigating treatment effects of participating jointly in SNAP and WIC when the treatment is validated only for SNAP. Southern Economic Journal, 86(1), 124-155. Similarly, participation in both SNAP and WIC as a young child may increase the odds of being more food secure in young adulthood than in childhood compared to low-income children who do not participate in either SNAP or WIC. See Wolfson J, Insolera N, Cohen A (2019). The influence of nutrition assistance program participation, parental nutritional knowledge, and family foodways on food security and child well-being. University of Kentucky Center for Poverty Research Discussion Paper Series, DP2019-02. University of Kentucky Center for Poverty Research.
[86] Arteaga I, Heflin C, Gable S (2016). The impact of aging out of WIC on food security in households with children. Children and Youth Services Review, 69:82-96.
[87] Metallinos-Katsaras E, Gorman KS, Wilde P, Kallio J (2011). A longitudinal study of WIC participation on household food insecurity. Journal of Maternal and Child Health, 15(5):627-633.
[88] Bersak T, Sonchak L (2018). The impact of WIC on infant immunizations and healthcare utilization. Health Services Research, 53.S1:2952-2969.
[89] Thomas TN, Kolasa MS, Zhang F, Shefer AM (2014). Assessing immunization interventions in the women, infants, and children (WIC) program. American Journal of Preventive Medicine, 47(5):624-628.
[90] Borger et al. (2020) op. cit.
[91] Buescher P et al. (2003). Child participation in WIC: Medicaid costs and use of health care services. American Journal of Public Health, 93(1):145-150; Chatterji P, Brooks-Gunn J (2004). WIC participation, breastfeeding practices, and well-child care among unmarried, low-income mothers. American Journal of Public Health, 94(8):1324-1327; Bersak and Sonchak (2018). One study (Chorniy, Currie, Sonchak L 2020) found no difference in access to health care between WIC children and non-WIC siblings within families. If, however, all children in a family benefit when one child gains access to health care, these estimates could underestimate WIC’s true impact on health care utilization.
[92] Anderson, PM, Butcher, KF, and Schanzenbach, DW (2019). Understanding recent trends in childhood obesity in the United States. Economics & Human Biology, 34:16-25.
[93] Fryar CD, Carroll MD, Ogden CL (2018). Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2–19 years: United States, 1963–1965 through 2015–2016. National Center for Health Statistics, September.
[94] Pan L, Freedman DS, Park S, Galuska DA, Potter A, Blanck, H. M. (2019). Changes in obesity among US children aged 2 through 4 years enrolled in WIC during 2010-2016. Journal of the American Medical Association, 321(23), 2364-2366; Pan L, Blanck HM, Park S, Galuska DA, Freedman DS, Potter A, Petersen R (2019). State-specific prevalence of obesity among children aged 2–4 years enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children—United States, 2010–2016. Morbidity and Mortality Weekly Report, 68(46):1057.
[95] Baker RD, Greer FR, Committee on Nutrition (2010). Clinical report — Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age). Pediatrics, 126(5):1040-1050.
[96] Butte NF, Fox MK, Briefel, RR, Siega-Riz AM, Dwyer JT, Deming DM, Reidy KC. (2010). Nutrient intakes of US infants, toddlers, and preschoolers meet or exceed dietary reference intakes. Journal of the American Dietetic Association, 110(12):S27-S37.
[97] Yip R, Binkin NJ, Fleshood L, Trowbridge FL (1987). Declining prevalence of anemia among low-income children in the United States. Journal of the American Medical Association, 258(12):1619-1623; Yip R, Parvanta I, Scanlon K, Borland E, Russell C, Trowbridge F (1992). Pediatric nutrition surveillance system — United States, 1980-1991. Morbidity and Mortality Weekly Report, 41(7):1-24.
[98] Yen ST (2010). The effects of SNAP and WIC programs on nutrient intakes of children. Food Policy, 35(6):576-583; and Siega-Riz AM, Kranz S, Blanchette D, Haines PS, Guilkey DK, Popkin BM (2004). The effect of participation in the WIC program on preschoolers’ diets. The Journal of Pediatrics, 144(2):229-234.
[99] Jun S, Catellier DJ, Eldridge AL, Dwyer JT, Eicher-Miller HA, Bailey RL (2018). Usual nutrient intakes from the diets of US children by WIC participation and income: findings from the Feeding Infants and Toddlers Study (FITS) 2016, The Journal of Nutrition, 148(Suppl_3):1567S–1574S.
[100] U.S. Department of Agriculture, Food and Nutrition Service (2012). National Survey of WIC Participants II: Participant Characteristics Report, prepared by ICF Macro for the Office of Research and Analysis, https://www.fns.usda.gov/national-survey-wic-participants-ii.
[101] Jackson MI (2015). Early childhood WIC participation, cognitive development and academic achievement. Social Science & Medicine, 126:145-153, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4703081/. There is some evidence that brief gaps in coverage may have short-term but not long-term consequences for achievement. Children who enter kindergarten after aging out of WIC and experience a gap in nutrition assistance coverage score lower on math and reading tests in the fall of their kindergarten year, but not in the spring (see Arteaga et al. (2019). Design flaws: consequences of the coverage gap in food programs on children at kindergarten entry. Applied Economic Perspectives and Policy, 41(2): 265-283. Another study that focused on socioemotional rather than cognitive development in a small sample of Medicaid recipients in Memphis, TN found no association between WIC participation at 12 and 24 months and an assessment of infants’ and toddlers’ socioemotional competence and behavioral problems; see Arons A, Bolbocean C, Bush NR, Tylavsky FA, LeWinn KZ (2016). Participation in the special supplemental nutrition program for women, infants, and children is not associated with early childhood socioemotional development: results from a longitudinal cohort study. Preventive Medicine Reports, 4:507511, http://www.sciencedirect.com/science/article/pii/S2211335516301103.
[102] Chorniy, Currie, Sonchak L (2020) op. cit. Note that some of those whose mothers participated during pregnancy may also have received WIC benefits as children. Among children in South Carolina who were covered prenatally, 89.3 percent continued to receive WIC services in their first year of life, dropping to 60.6 percent, 42.8 percent, 31.0 percent, and 22.0 percent in the four years that follow.
[103] Although the evidence is at best anecdotal, food manufacturers may also respond to WIC’s food package requirements by reformulating their products. In the mid-1980s, for example, General Mills increased the amount of iron in Cheerio s— one of the most popular WIC-eligible cereals — so that it would meet program requirements.
[104] Ploeg MV, Breneman V, Farrigan T, Hamrick K, Hopkins D, Kaufman P, Lin BH, Tuckermanty E (2009). Access to Affordable and Nutritious Food: Measuring and Understanding Food Deserts and Their Consequences. Report to Congress. Economic Research Service, USDA, https://www.ers.usda.gov/webdocs/publications/ap036/12716_ap036_1_.pdf.
[105] USDA reports that about 1 in 5 WIC households live more than a mile from a supermarket in urban areas and more than 10 miles from a supermarket in rural areas. Nearly 90 percent of mothers agree, however, that fresh fruits and vegetables are easy to purchase and plentiful in their communities. See Borger et al. (2020) op. cit.
[106] An examination of rules in place in 2017 found a wide range of minimum stocking requirements for WIC-authorized retailers across states, which may result in disparities in food and beverage products available to WIC recipients depending on their state of residence and the size or type of stores available in their neighborhoods. See Pelletier JE, Schreiber LR, Laska MN (2017). Minimum stocking requirements for retailers in the Special Supplemental Nutrition Program for Women, Infants, and Children: disparities across US states. American Journal of Public Health, 107(7), 1171-1174.
[107] Tiehen L Frazão E (2016). Where Do WIC Participants Redeem Their Food Benefits? An Analysis of WIC Food Dollar Redemption Patterns by Store Type. Economic Research Service, USDA, https://www.ers.usda.gov/webdocs/publications/eib152/57246_eib152.pdf.
[108] Andreyeva T, Luedicke J, Middleton AE, Long MW, Schwartz MB (2012). Positive influence of the revised Special Supplemental Nutrition Program for Women, Infants, and Children food packages on access to healthy foods. Journal of the Academy of Nutrition and Dietetics, 112(6):850-858; Havens EK, Martin KS, Yan J, Dauser-Forrest D, Ferris AM (2012). Federal nutrition program changes and healthy food availability. American Journal of Preventive Medicine, 43(4):419-422.
[109] Hillier A, McLaughlin J, Cannuscio CC, Chilton M, Krasny S, Karpyn A (2012). The impact of WIC food package changes on access to healthful food in 2 low-income urban neighborhoods. Journal of Nutrition Education and Behavior, 44(3):210-216.
[110] Rose D, O’Malley K, Dunaway LF, Bodor JN (2014). The influence of the WIC food package changes on the retail food environment in New Orleans. Journal of Nutrition Education and Behavior, 46(3 Supplement):S38-44.
[111] Zenk SN, Odoms-Young A, Powell LM, Campbell RT, Block D, Chavez N, Krauss RC, Strode S, Armbruster J (2012). Fruit and vegetable availability and selection: federal food package revisions, 2009. American Journal of Preventive Medicine, 43(4):423-428.
[112] Gleason S, Morgan R, Bell L, Pooler J (2011). Impact of the Revised WIC Food Package on Small WIC Vendors. Alexandria, VA: Altarum Institute, http://altarum.org/sites/default/files/uploaded-related-files/FourStateWICFoodPackageEvaluation-Exec%20Summary-22Mar11_0.pdf.
[113] Cobb LK, Anderson CA, Appel L, JonesSmith J, Bilal U, Gittelsohn J, Franco M (2015). Baltimore City stores increased the availability of healthy food after WIC policy change. Health Affairs, 34(11):18491857.
[114] Lu W, McKyer DL, Dowdy D, Evans A, Ory M, Hoelscher DM, Wang S, Miao J (2016). Evaluating the influence of the revised Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food allocation package on healthy food availability, accessibility, and affordability in Texas. Journal of the Academy of Nutrition and Dietetics, 116(2):292-301.
[115] Hudak KM, Paul R, Gholizadeh S, Zadrozny W, Racine EF (2020). Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) authorization of discount variety stores: leveraging the private sector to modestly increase availability of healthy foods. The American Journal of Clinical Nutrition, 111(6): 1278-1285.
[116] Chauvenet C, De Marco M, Barne, C, Ammerman AS (2019). WIC recipients in the retail environment: a qualitative study assessing customer experience and satisfaction. Journal of the Academy of Nutrition and Dietetics, 119(3), 416-424. Many of the interviews in this study were conducted in states prior to the implementation of Electronic Benefit Transfer (EBT) systems and mobile phone applications to help with WIC shopping. Participants who had experience with EBT reported a smoother checkout process since EBT’s implementation.
[117] See, for example, Besharov DJ, Germanis P (2001). Rethinking WIC: An Evaluation of the Women, Infants, and Children Program. Washington, DC: American Enterprise Institute.
[118] Bitler MP, Currie J (2005). Does WIC work? The effects of WIC on pregnancy and birth outcomes. Journal of Policy Analysis and Management, 24(1):73-91.
[119] Joyce T, Racine A, Yunzal‐Butler C (2008). Reassessing the WIC effect: evidence from the pregnancy nutrition surveillance system. Journal of Policy Analysis and Management, 27(2):277-303.
[120] Fingar KR, Lob SH, Dove MS, Gradziel P, Curtis MP (2016). Reassessing the association between WIC and birth outcomes using a fetusesatrisk approach. Maternal and Child Health Journal, published online August 16, 2016.
[121] Nobles J, Hamoudi, A (2019). Detecting the effects of early-life exposures: why fecundity matters. Population Research and Policy Review, 38(6), 783-809.
More from the Authors

Steven Carlson is a research analyst who previously directed the Office of Policy Support at the Agriculture Department’s Food and Nutrition Service.
