
OMB ESTIMATES INDICATE THAT
900,000 CHILDREN WILL LOSE
HEALTH INSURANCE DUE TO
REDUCTIONS IN FEDERAL SCHIP FUNDING
Congress Could Extend
the Availability of Expiring SCHIP Funds and
Undo the Reduction in SCHIP
Funding Levels to Avert a Large Enrollment Decline
by
Edwin Park, Leighton Ku and Matthew Broaddus
|
PDF
of this report Related Analyses |
| If you cannot access the files through the links, right-click on the underlined text, click "Save Link As," download to your directory, and open the document in Adobe Acrobat Reader. |
Federal funding for the State Children’s Health Insurance Program (SCHIP) dropped by 26 percent, or more than $1 billion, in fiscal year 2002 and is scheduled to remain at this level in each of the next two fiscal years. The Balanced Budget Act of 1997, which established SCHIP, included this reduction solely to ensure the budget was balanced by 2002 under the budget and economic assumptions in use at that time. However, because of this funding reduction and rising SCHIP enrollments and expenditures, a substantial number of states are expected to have insufficient federal funds available to sustain their SCHIP programs in the years ahead.
As a result, the number of children insured through SCHIP is expected to fall over the next several years. While it is often assumed that states have sufficient federal SCHIP funding because billions of dollars in unspent SCHIP funds from prior years are currently available, these unspent SCHIP funds are not excess funds. To the contrary, states need these unspent funds to help offset the effects of the SCHIP funding reduction while covering the ongoing costs of their SCHIP programs. Despite the presence of these unspent funds, the Office of Management and Budget projects that national SCHIP enrollment will decline by 900,000 children between 2003 and 2006 (see Figure 1).
Even as states face funding shortfalls, a total of $2.7 billion of the unspent federal SCHIP funds are scheduled to expire and revert to the Treasury at the end of either fiscal year 2002 or fiscal year 2003. Under current law, states that have unspent SCHIP funds made available through a reallocation process must return those funds to the U.S. Treasury if they do not use them within a limited period of time. The expiring funds are the result of both targeting and timing problems associated with the SCHIP reallocation system. Some states have unspent funds available to them that they are not likely ever to use. Other states with unspent SCHIP funds that are scheduled to revert to the Treasury are expected to have insufficient federal funds over the next several years to maintain their SCHIP enrollments; there is a mismatch in these states between the time for which the unspent funds have been provided to states and must be used to prevent the funds from reverting to the Treasury and the time when the states will need these funds to avert cutbacks in their SCHIP programs. Some $1.2 billion of unspent SCHIP funds reverted to the Treasury on September 30, 2002. An additional $1.5 billion are expected to revert to the Treasury on September 30, 2003.
An effective approach to address this problem would be to restore the SCHIP funding levels for fiscal years 2003 and 2004 to its normal level and to extend the expiring funds and target those funds to states that need them and are most likely to use them. Bipartisan legislation introduced in the Senate would do that. If this is done, the vast majority of the substantial enrollment decline that threatens the success of the SCHIP program can be averted.
The Scheduled SCHIP Funding Reduction and Its Effect on Children’s Enrollment
When Congress created SCHIP in 1997, it provided states with $40 billion over ten years to expand health care coverage for low-income uninsured children.[1] Under the 1997 legislation, however, the annual level of SCHIP funding drops substantially for fiscal year 2002 and the two subsequent fiscal years. Congress intended to balance the budget by 2002. To help achieve that goal, the Balanced Budget Act of 1997 — which created SCHIP — included a reduction in funding levels for several programs in 2002, including SCHIP. Without these reductions, that legislation would have fallen short of balancing the budget in 2002, under the economic and budget assumptions in use at the time the legislation was enacted.
SCHIP funding is scheduled to drop by more than $1 billion, or 26 percent, in fiscal year 2002. It is slated to remain at this reduced level through the end of fiscal year 2004 (see Figure 2).
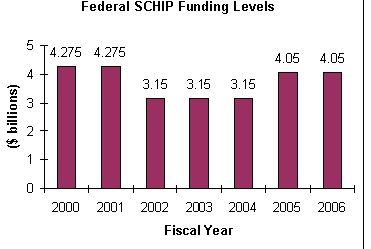
Unfortunately, this funding reduction is taking effect at a time that many states have an increased need for SCHIP funds. Although states confronted a series of implementation challenges when they first established their SCHIP programs and SCHIP consequently got off to a slow start, SCHIP enrollment has been increasing sharply in the past few years.[2] Federal SCHIP expenditures have climbed correspondingly, jumping from $200 million in fiscal year 1998, the program’s first year, to $600 million in fiscal year 1999, $1.8 billion in fiscal year 2000, and $2.7 billion in fiscal year 2001.[3] OMB estimates that federal SCHIP expenditures will reach $4.3 billion in fiscal year 2003. (Similarly, CBO estimates that SCHIP expenditures will reach $4.5 billion in fiscal year 2003.) Yet, federal SCHIP funding will be only $3.15 billion each year for fiscal years 2002 through 2004.
It is possible, using the SCHIP expenditure and funding projections of the Centers for Medicare and Medicaid Services at the U.S. Department of Health and Human Services to analyze how the reduction in SCHIP funding will affect states in the years ahead.[4] Such an analysis indicates that in a growing number of states, SCHIP expenditures will outpace the annual federal SCHIP allotment that the state receives. Some 29 states are expected to achieve a level of SCHIP expenditures in fiscal year 2003 that exceeds their fiscal year 2003 allotments (see Table 1). As noted, total SCHIP expenditures nationally are projected to be $4.3 billion in 2003 according to OMB and $4.5 billion according to CBO, even though only $3.15 billion in federal SCHIP funds will be allocated.
|
Twenty States Will Have Insufficient Federal Funding to
According to our estimates based on the CMS model, under current law, the following 20 states will face federal funding shortfalls some time between now and fiscal year 2007: Alaska, Arizona, California, Florida, Georgia, Iowa, Kansas, Kentucky, Louisiana, Maryland, Minnesota, Mississippi, Missouri, New Jersey, New York, Rhode Island, South Dakota, Texas, West Virginia and Wisconsin. |
In most cases, these states can turn to unspent SCHIP funds currently available from prior years to offset the shortfalls associated with their fiscal year 2003 allotments. After 2003, however these unspent funds from the earlier years of SCHIP will start to run out in many of these states. (And as noted, $2.7 billion of these funds are scheduled to revert to the Treasury by the end of fiscal year 2003; see Table 2.) By fiscal year 2007, the level of federal SCHIP funding needed to sustain states’ projected SCHIP enrollment will exceed the total federal SCHIP funds available, including unspent funds from prior years and funds reallocated from other states, in 20 states (see Table 3). In many areas, the magnitude of the shortfalls will be very large. By fiscal year 2006, the level of funding needed to sustain enrollment will be more than twice the total SCHIP funds available in nine states. In the years ahead, these states will have to reduce the number of children they insure through SCHIP, unless they provide additional funds from state treasuries.
Given the serious fiscal problems many states are now experiencing, the provision of additional state funds is unlikely in many areas. If the affected states are unable (or unwilling) to increase state funding to compensate, they will have no choice but to cut their SCHIP programs, thereby increasing the numbers of low-income children who are uninsured.
A large number of children thus are expected to lose out on coverage. According to OMB, despite the current availability of unspent funds from prior years, the increase in the number of children enrolled in SCHIP programs nationally will slow markedly in fiscal year 2003 as the effects of the SCHIP funding reduction begin to be felt, and SCHIP enrollment will start declining after 2003. OMB projects that SCHIP enrollment will reach 4.3 million in 2003 but fall to 4.1 million in 2004, 3.6 million in 2005, and 3.4 million in 2006 (see Figure 1). That constitutes a decline of 900,000 children over three years.[5]
|
Any Extension of Expiring SCHIP Funds Must Target Those
Funds to
States Projected to Have Federal Funding Shortfalls
An essential element of any extension of the
$2.7 billion in expiring funds is that the funds be made available to
states projected to have insufficient federal SCHIP funding.
This will ensure that the funds can be used by those states to
lessen and/or delay funding shortfalls and as a result, avert large
enrollment declines.
An extension of expiring funds that does not primarily target the states most in need of additional federal funding would do little to reduce the national enrollment decline projected by OMB. For example, if the availability of the funds scheduled to revert to the Treasury were extended but left entirely in the states expected to lose such funds, this would leave a large portion of the expiring funds in states not likely ever to use them fully. This is because 15 of the 21 states that had unspent funds expire and revert to the Treasury at the end of fiscal year 2002 and four of the 11 states expected to have funds revert to the Treasury at the end of fiscal year 2003 are not projected to have insufficient federal funds in the years ahead (see Tables 2 and 3). Under such an untargeted extension, only a few of the states projected to have funding shortfalls would gain sufficient additional federal funding to maintain their SCHIP enrollments. Such an approach would produce only a modest reduction in the projected national SCHIP enrollment decline. |
Moreover, with a number of states concerned that their future SCHIP costs will outstrip their available federal funding, some states may take steps to halt or slow increases in SCHIP enrollment before the year in which they will actually face a funding shortfall, causing fewer children to be insured in the interim than would otherwise be the case. Some states are likely to start taking such steps in 2003 to avoid having to cut the number of children insured through SCHIP in subsequent years.[6]
Extending the Expiring Funds and Restoring Federal Funding to Avert the Enrollment Decline
Despite the federal SCHIP funding reduction, a total of $2.7 billion either expired and reverted to the Treasury at the end of fiscal year 2002 or is projected to do so at the end of fiscal year 2003. No SCHIP funds are projected to expire and revert to the Treasury in years after 2003.[7]
Under current law, states that have unspent fiscal year 1998 and fiscal year 1999 funds must return those funds to the U.S. Treasury if they did not use them by September 30, 2002. In addition, states receiving unspent fiscal year 2000 funds this year that have been reallocated from other states must return those funds to the U.S. Treasury if they do not expend them by the end of September 30, 2003.
Unfortunately, there are significant targeting and timing problems associated with the SCHIP reallocation process. Some states were never expected to use all of their unspent fiscal year 1998 and fiscal year 1999 funds. Other states will not be able to use all of the funds made available to them through the reallocation process within the required timeframe under federal law, because of a mismatch between the time when these unspent funds are available to these states and the time when these states are projected to have SCHIP funding shortfalls and to need the funds. For example, some of the SCHIP programs that will lose unspent funds at the end of fiscal year 2002 and fiscal year 2003 will badly need those expiring funds in later years.
The Administration has recognized the need to extend the expiring funds to help avert the projected national enrollment decline. The Administration’s fiscal year 2003 budget includes a proposal to extend until the end of fiscal year 2006 the availability of the expiring funds. Yet, the proposal is significantly flawed because it does little to avert the looming SCHIP enrollment decline for two primary reasons: it does not restore overall SCHIP funding and it leaves large sums of SCHIP funds in states that cannot use them rather than redistributing the funds to other states that will need them to avert sharp cutbacks in their SCHIP programs. Under the Administration’s proposal, 17 states would still face federal funding shortfalls at some point between now and 2007. As a result, 515,000 children would lose their health insurance coverage between 2003 and 2007. In addition, the Administration’s plan would have an immediate adverse effect on SCHIP enrollment: 200,000 fewer children would be enrolled in 2003 than would be enrolled under current law, because several states that would receive sufficient funds in 2003 as a result of a reallocation scheduled under current law would have insufficient funds under the Administration plan, which would cancel that reallocation.[8]
Senators Jay Rockefeller (D-WV), Lincoln Chafee (R-RI), Edward Kennedy (D-MA) and Orrin Hatch (R-UT) have introduced bipartisan legislation (S. 2860) that would extend the availability of expiring SCHIP funds but target them to states that will most need these funds. The legislation meets this goal by strengthening the current reallocation system through establishment of a caseload stabilization pool under which certain unused SCHIP funds, including the funds that were scheduled to expire on September 30, 2002 and September 30, 2003, would be allocated to the states that need these funds to sustain their programs. This legislation also would restore overall federal SCHIP funding for fiscal years 2003 and 2004 to the annual levels provided for SCHIP in fiscal years 1998 through 2001.
Unlike the Administration proposal, this legislation would halve the number of states expected to have insufficient federal funds by 2007 and result in no states having insufficient SCHIP funds to maintain enrollment until at least 2005. Moreover, the national SCHIP enrollment decline between 2003 and 2007 would be reduced by 75 percent. As a result, this legislation represents a much more effective proposal than the Administration proposal in preserving children’s health insurance coverage.[9]
In addition, on October 1, Senators Max Baucus (D-MT) and Charles Grassley (R-IA) — the chairman and ranking minority member of the Senate Finance Committee — introduced legislation (S. 3018) related to Medicare provider reimbursements that includes SCHIP funding provisions. The Baucus-Grassley legislation incorporates some but not all of the elements of S. 2860. (It does not restore SCHIP funding levels for fiscal years 2003 and 2004 to the earlier SCHIP funding levels, and it makes some other modifications to S. 2860.) While significantly less effective than the Rockefeller-Chafee-Kennedy-Hatch bill in averting the SCHIP enrollment decline, the Baucus-Grassley proposal includes the proposal for a caseload stabilization pool. This would help avert nearly the entire national coverage decline through 2006, a substantially better outcome than would occur under the Administration proposal.[10] However, under the Baucus-Grassley proposal, a sizable enrollment reduction would nonetheless result by 2007.[11]
Conclusion
Due to a 26 percent reduction in federal SCHIP funding in 2002 and over the next two years, the scheduled expiration of several billion dollars in SCHIP funds and a mismatch between the states in which some SCHIP funds are located and the states that will these funds to avert cutbacks, a number of states will face significant SCHIP funding shortfalls over the next several years and be unable to sustain their SCHIP enrollments. OMB projects a national SCHIP enrollment decline of 900,000 children between 2003 and 2006. States consequently are greatly in need of the estimated $2.7 billion in federal SCHIP funds that were scheduled to expire and revert to the Treasury at the end of fiscal year 2002 and fiscal year 2003.
Extending the availability of the expiring funds, placing those funds in the states that need them, and restoring full federal SCHIP funding for the next two years would permit many more states to maintain their enrollments and avert much of the national SCHIP enrollment decline. Congress has the ability to approve such SCHIP funding initiatives during the post-election lame-duck session that will occur this month or in December. Doing so would maintain SCHIP’s successful work in providing health insurance to millions of low-income uninsured children.
|
State |
Projected FY 2003 SCHIP Expenditures as Percent of FY 2003 SCHIP Allotment |
|
|
|
|
|
|
Alabama |
138% |
|
|
Alaska |
378% |
|
|
Arizona |
238% |
|
|
Colorado |
129% |
|
|
Florida |
188% |
|
|
Georgia |
174% |
|
|
Indiana |
125% |
|
|
Iowa |
181% |
|
|
Kansas |
160% |
|
|
Kentucky |
217% |
|
|
Louisiana |
140% |
|
|
Maine |
164% |
|
|
Maryland |
427% |
|
|
Massachusetts |
134% |
|
|
Minnesota |
206% |
|
|
Mississippi |
250% |
|
|
Missouri |
186% |
|
|
Montana |
106% |
|
|
New Jersey |
454% |
|
|
New York |
244% |
|
|
North Carolina |
127% |
|
|
Ohio |
123% |
|
|
Pennsylvania |
122% |
|
|
Rhode Island |
476% |
|
|
South Carolina |
130% |
|
|
South Dakota |
183% |
|
|
Texas |
167% |
|
|
West Virginia |
162% |
|
|
Wisconsin |
206% |
|
| * Updated November 2002 analysis based on the SCHIP expenditure and funding model used by the Centers for Medicare and Medicaid Services and using fiscal year 2002 expenditures and state estimates of fiscal year 2003 expenditures as reported to CMS as of August 2002 as well as actual fiscal year 2003 base allotments. The model has been modified to reflect more accurate state expenditure sequences (this refers to the order in which states spend their annual SCHIP allotments and the SCHIP funds made available to states through the reallocation process), incorporate expenditure estimates under recently approved section 1115 waivers in Arizona, California, Colorado, Illinois and Oregon that use SCHIP funds to expand coverage to adults and/or pregnant women, and use CBO estimates for the rate of growth in per-capita health care costs for children. | ||
|
State |
Unspent SCHIP Funds |
Unspent SCHIP Funds |
|
|
|
|
|
National Total |
$1,209.6 |
$1,505.4 |
|
Alaska |
$9.9 |
— |
|
Arkansas |
$44.6 |
— |
|
Delaware |
$2.1 |
— |
|
Hawaii |
$2.5 |
— |
|
Illinois |
$21.9 |
— |
|
Indiana |
$105.2 |
— |
|
Kansas |
— |
$70.3 |
|
Kentucky |
$58.2 |
$122.2 |
|
Maine |
$15.4 |
$34.6 |
|
Maryland |
$38.0 |
$58.4 |
|
Massachusetts |
$65.7 |
$121.4 |
|
Mississippi |
— |
$112.4 |
|
Montana |
— |
$34.9 |
|
New Hampshire |
$4.0 |
— |
|
New Mexico |
$42.5 |
— |
|
New York |
$526.5 |
$526.2 |
|
North Carolina |
$92.1 |
— |
|
Oklahoma |
$7.1 |
— |
|
Rhode Island |
$1.3 |
— |
|
South Carolina |
$115.9 |
$189.0 |
|
Tennessee |
$15.2 |
— |
|
Washington |
$36.1 |
— |
|
West Virginia |
— |
$45.6 |
|
Wisconsin |
$2.8 |
$80.0 |
|
Wyoming |
$1.4 |
— |
|
Territories |
$1.2 |
$110.4 |
| * Total available SCHIP funds include annual allotments available to the state and any additional funds made available through the SCHIP reallocation process. Updated November 2002 analysis based on SCHIP expenditure and funding model used by the Centers for Medicare and Medicaid Services with CBPP modifications and using fiscal year 2002 expenditures and state estimates of fiscal year 2003 expenditures, as reported to CMS as of August 2002. | ||
|
State |
FY 2003 |
FY 2004 |
FY 2005 |
FY 2006 |
FY 2007 |
|
|
|
|
|
|
|
|
Alaska |
|
60% |
33% |
31% |
36% |
|
Arizona |
|
85% |
42% |
38% |
44% |
|
California |
|
|
|
|
97% |
|
Florida |
|
|
83% |
54% |
62% |
|
Georgia |
|
|
96% |
49% |
57% |
|
Iowa |
|
|
|
75% |
67% |
|
Kansas |
|
|
|
|
79% |
|
Kentucky |
|
|
|
62% |
62% |
|
Louisiana |
|
|
|
|
77% |
|
Maryland |
|
73% |
26% |
25% |
28% |
|
Minnesota |
|
|
61% |
50% |
58% |
|
Mississippi |
|
|
54% |
37% |
43% |
|
Missouri |
|
|
|
64% |
65% |
|
New Jersey |
|
82% |
63% |
74% |
98% |
|
New York |
|
|
68% |
42% |
48% |
|
Rhode Island |
|
60% |
21% |
20% |
23% |
|
South Dakota |
|
|
75% |
47% |
55% |
|
Texas |
|
|
|
67% |
63% |
|
West Virginia |
|
|
|
|
99% |
|
Wisconsin |
|
|
87% |
49% |
57% |
| * Total available SCHIP funds include annual allotments available to the state and any additional funds made available through the SCHIP reallocation process. Updated November 2002 analysis based on SCHIP expenditure and funding model used by the Centers for Medicare and Medicaid Services with CBPP modifications and using fiscal year 2002 expenditures and state estimates of fiscal year 2003 expenditures, as reported to CMS as of August 2002, as well as actual fiscal year 2003 base allotments. | |||||
End Notes:
[1] Under SCHIP, states can use SCHIP funds to provide health insurance to low-income uninsured children through either Medicaid or a separate state health insurance program. The total amount of SCHIP funds available each year is divided among the states (and territories) according to a formula in the SCHIP statute. States have three years to use the SCHIP allotment they receive for a particular year. If a state is unable to use its allotment within the three-year period, its unused funds are reallocated to states that did use their full allotment for that year. (Special rules apply for fiscal years 1998 and 1999.)
These federal funds are distributed to states on a “matching” basis. Under the matching formula, the federal government picks up between 65 percent and 85 percent of the cost of covering a child, depending on the state. Each state’s matching rate is equal to its Medicaid matching rate plus 30 percent of the difference between the Medicaid rate and 100 percent. In essence, the SCHIP matching rate reduces a state’s share of the cost of financing children’s health insurance by 30 percent, as compared to the state’s share under the regular Medicaid program.
[2] For example, the Centers for Medicare and Medicaid Services estimated that a total of 4.6 million children were enrolled in SCHIP at some point in fiscal year 2001. Two years earlier, in fiscal year 1999, there were two million children ever enrolled in SCHIP and in fiscal year 2000, there were 3.3 million children ever enrolled in SCHIP. Centers for Medicare and Medicaid Services, The State Children’s Health Insurance Program Annual Enrollment Report, February 6, 2002. OMB estimates differ from CMS estimates because the OMB enrollment estimates use an annual average, rather than the total number of children who are ever enrolled during the course of a year. OMB determined that average annual enrollment was 2.1 million in fiscal year 2000 and that enrollment rose by nearly 50 percent to 3 million in fiscal year 2001. (CBO does not provide SCHIP enrollment estimates.)
[3] As used here, the term “SCHIP expenditures” means the federal share of expenditures for health insurance programs funded through SCHIP, while the term “SCHIP funds” refers to federal SCHIP funding. The 2001 figure has been adjusted downward from $3.7 billion because that figure reflected a one-time technical fix in that year that artificially inflated spending for baseline purposes.
[4] Our initial May 2002 analysis of how states will be affected has now been updated. This November 2002 updated analysis continues to be based on a state-specific SCHIP expenditure and funding model provided by the Centers for Medicare and Medicaid Services but now uses fiscal year 2002 expenditures and state estimates of fiscal year 2003 expenditures reported to CMS as of August 2002. We modify the CMS model to reflect more accurate state expenditure sequences (this refers to the order in which states spend their annual SCHIP allotments and the SCHIP funds made available to states through the reallocation process), incorporate expenditure estimates under recently approved section 1115 waivers in Arizona, California, Colorado, Illinois and Oregon that use SCHIP funds to expand coverage to adults and/or pregnant women, and use CBO estimates for the rate of growth in per-capita health care costs for children.
States in which total SCHIP funds will become insufficient to maintain caseloads some time between now and fiscal year 2007 include: Alaska, Arizona, California, Florida, Georgia, Iowa, Kansas, Kentucky, Louisiana, Maryland, Minnesota, Mississippi, Missouri, New Jersey, New York, Rhode Island, South Dakota, Texas, West Virginia and Wisconsin.
Our initial May 2002 analysis included Idaho and Indiana among the states projected to have insufficient funds and did not include California, Florida, Georgia and South Dakota.
[5] Office of Management and Budget, Analytical Perspectives, Budget of the United States Government, Fiscal Year 2003, p.297.
Under our model, projected enrollment in 2003 under current law would be about 4.5 million and the projected decline in national SCHIP enrollment between 2003 and 2007 would be 800,000 to 3.7 million, a bit smaller than OMB’s projected decline of 900,000. These numbers are not directly comparable to the original OMB enrollment estimates because of adjustments made to the data and projections from the Centers for Medicare and Medicaid Services and the use of a longer time period for analyzing national SCHIP enrollment trends (2003 through 2007); see footnote 4.
[6] While not cutting SCHIP enrollment of children, New Jersey recently cited fiscal pressures and insufficient federal SCHIP funding to sustain its SCHIP enrollment as the reasons for suspending new enrollment of low-income parents under its SCHIP waiver program. The suspension took effect on June 15, 2002. New Jersey Department of Human Services, Press Release, May 29, 2002.
[7] In its fiscal year 2003 budget issued in early February, the Department of Health and Human Services estimated that $3.2 billion in SCHIP funds would revert to the Treasury over the next two years. Due to greater-than-expected SCHIP expenditures in certain states in fiscal year 2002, likely as a result of the economic downturn, and new data on the sequence in which states access their federal funds, the amount of unexpended funds scheduled to revert to the Treasury is now expected to be somewhat smaller under our estimates.
[8] See Edwin Park and Matthew Broaddus, 515,000 Children Would Lose Health Insurance Over the Next Five Years under Flawed Administration SCHIP Proposal, Center on Budget and Policy Priorities, revised November 7, 2002.
[9] Under S. 2860, projected enrollment in 2007 would be about 4.3 million, as compared to 3.7 million under the Administration’s proposal.
[10] Under S. 3018, the projected enrollment in 2006 would be about 4.5 million, essentially the same level as in 2003. This is a significantly better outcome than under the Administration proposal; enrollment under that proposal would be about 4 million in 2006, a decline between 2003 and 2006 of more than 200,000. (Under the Administration’s proposal, enrollment in fiscal year 2003 was already reduced by 200,000). In contrast to the other proposals, the Rockefeller-Chafee-Kennedy-Hatch legislation (S. 2860) would result in projected enrollment of about 4.8 million in 2006, an increase between 2003 and 2006 of 375,000.
[11] Because S. 3018 does not restore SCHIP funding levels for fiscal year 2003 and 2004 to the earlier SCHIP funding levels and the funds available to the caseload stabilization pool for additional redistributions are exhausted by the end of 2006, a growing number of states will face more significant shortfalls in 2007 and as a result, projected enrollment under S. 3018 would decline to about 4 million in 2007.